

Cannulation strategies for extracorporeal membrane oxygenation
- PMID: 37525707
- PMCID: PMC10387010
- DOI: 10.1007/s12055-023-01537-0
Cannulation strategies for extracorporeal membrane oxygenation
Abstract
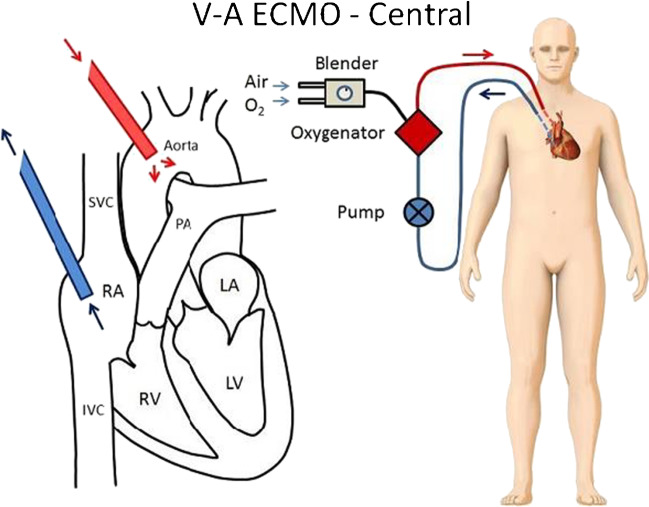
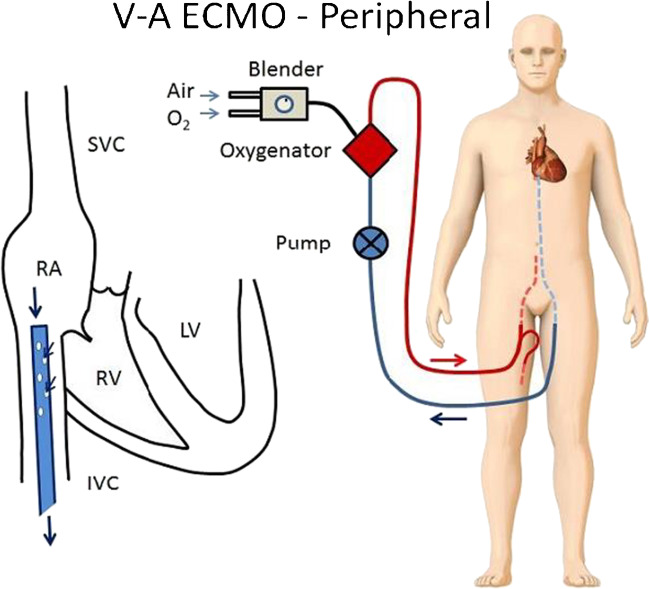
Extracorporeal membrane oxygenation (ECMO) is a type of extracorporeal life support (ECLS) in which the function of the heart and/or lungs is partially or completely replaced by a portable system that provides prolonged support to critically ill patients with respiratory or cardiac failure. There are two major variants of ECMO: veno-venous (VV) ECMO and veno-arterial (VA) ECMO. VV ECMO replaces the function of the lung in which it uses a cannula to remove venous blood and oxygenates it using the extracorporeal system, and returns the blood to the right atrium to be pumped to the body. VA ECMO is slightly different in that it replaces the function of the heart and lungs by returning oxygenated blood to the aorta. As a therapy for respiratory failure, ECMO minimizes hypoxia, diminishes lung stress and strain, and allows lung protective mechanical ventilation. As a support for acute and terminal heart failure, ECMO reduces preload, increases aortic flow, and allows for end-organ perfusion. Due to its physiological support and advantages, it is used for a variety of chronic and acute support purposes such as bridge therapy for heart/lung transplant, durable ventricular assist devices, and intermediate-term mechanical support postoperatively. Our review gives a broad overview of the two main types of ECMO strategies and their clinical indications, cannulation strategies, unique clinical utility, and their limitations.
Keywords: Cannulation; Cardiothoracic surgery; ECMO.
© Indian Association of Cardiovascular-Thoracic Surgeons 2023. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Conflict of interest statement
Conflict of interestAll authors report no conflict of interest.
Figures



References
-
- Naidu SS, Baran DA, Jentzer JC, Hollenberg SM, van Diepen S, Basir MB, et al. SCAI SHOCK Stage Classification Expert Consensus update: a review and incorporation of validation studies: This statement was endorsed by the American College of Cardiology (ACC), American College of Emergency Physicians (ACEP), American Heart Association (AHA), European Society of Cardiology (ESC) Association for Acute Cardiovascular Care (ACVC), International Society for Heart and Lung Transplantation (ISHLT), Society of Critical Care Medicine (SCCM), and Society of Thoracic Surgeons (STS) in December 2021. J Am Coll Cardiol. 2022;79:933–946. doi: 10.1016/j.jacc.2022.01.018. - DOI - PubMed
-
- Baran DA, Grines CL, Bailey S, Burkhoff D, Naidu SS, et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock. Catheter Cardiovasc Interv. 2019;94:29–37. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials