

Phase I trial of panobinostat in children with diffuse intrinsic pontine glioma: A report from the Pediatric Brain Tumor Consortium (PBTC-047)
- PMID: 37526549
- PMCID: PMC10708931
- DOI: 10.1093/neuonc/noad141
Phase I trial of panobinostat in children with diffuse intrinsic pontine glioma: A report from the Pediatric Brain Tumor Consortium (PBTC-047)
Abstract
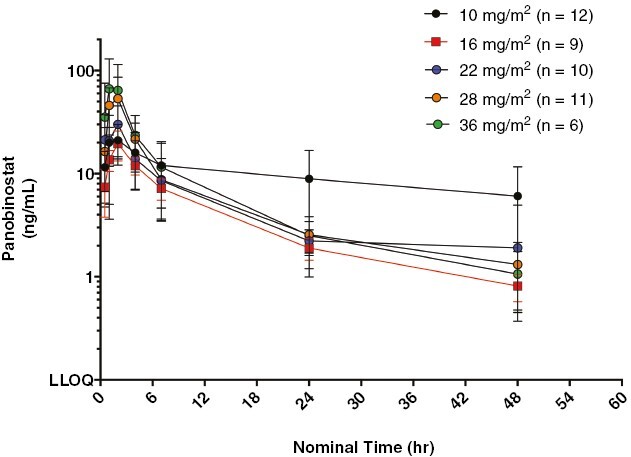
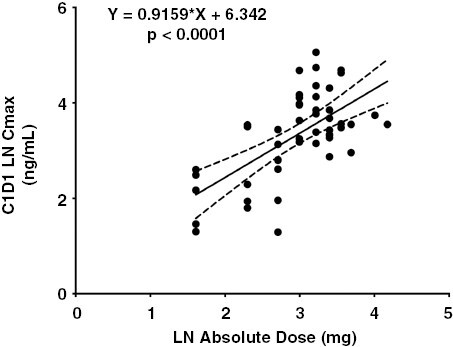
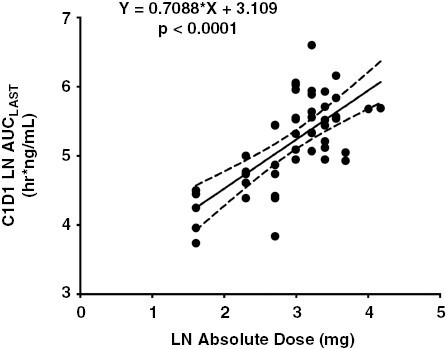
Background: Diffuse intrinsic pontine glioma (DIPG) is a lethal childhood cancer with median survival of less than 1 year. Panobinostat is an oral multihistone deacetylase inhibitor with preclinical activity in DIPG models. Study objectives were to determine safety, tolerability, maximum tolerated dose (MTD), toxicity profile, and pharmacokinetics of panobinostat in children with DIPG.
Patients and methods: In stratum 1, panobinostat was administered 3 days per week for 3 weeks on, 1 week off to children with progressive DIPG, with dose escalation following a two-stage continual reassessment method. After this MTD was determined, the study was amended to evaluate the MTD in children with nonprogressive DIPG/Diffuse midline glioma (DMG) (stratum 2) on an alternate schedule, 3 days a week every other week in an effort to escalate the dose.
Results: For stratum 1, 19 subjects enrolled with 17/19 evaluable for dose-finding. The MTD was 10 mg/m2/dose. Dose-limiting toxicities included thrombocytopenia and neutropenia. Posterior reversible encephalopathy syndrome was reported in 1 patient. For stratum 2, 34 eligible subjects enrolled with 29/34 evaluable for dose finding. The MTD on this schedule was 22 mg/m2/dose. DLTs included thrombocytopenia, neutropenia, neutropenia with grade 4 thrombocytopenia, prolonged intolerable nausea, and increased ALT.
Conclusions: The MTD of panobinostat is 10 mg/m2/dose administered 3 times per week for 3 weeks on/1 week off in children with progressive DIPG/DMG and 22 mg/m2/dose administered 3 times per week for 1 week on/1 week off when administered in a similar population preprogression. The most common toxicity for both schedules was myelosuppression.
Keywords: DIPG; HDAC inhibitors; brainstem glioma; epigenetics; midline glioma.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Michelle Monje served on the scientific advisory board for Cygnal Therapeutics and her family holds equity in Maplight Therapeutics; Ira J. Dunkel serves on the advisory board for AstraZeneca and Bristol Meyers Squibb and is a consultant for DAY One Therapeutics, Fennel, Glaxo Smith Kline, Pyramid and QED; Jason Fangusaro serves on the advisory board for Alexion/AstraZeneca and Merck; Katherine E. Warren serves on the advisory board for DAY One Therapeutics and Glaxo Smith Kline. All other authors have nothing to disclose.
Figures
References
-
- Schwartzentruber J, Korshunov A, Liu X, et al. Driver mutations in histone H3.3 and chromatin remodelling genes in paediatric glioblastoma. Nature. 2012;482(7384):226–231. - PubMed
-
- Jansen M, van Vuurden D, Vandertop W, Kaspers G.. Diffuse intrinsic pontine gliomas: a systematic update on clinical trials and biology. Cancer Treat Rev. 2012;38(1):27–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
