

Upfront Radiosurgery vs a Wait-and-Scan Approach for Small- or Medium-Sized Vestibular Schwannoma: The V-REX Randomized Clinical Trial
- PMID: 37526718
- PMCID: PMC10394573
- DOI: 10.1001/jama.2023.12222
Upfront Radiosurgery vs a Wait-and-Scan Approach for Small- or Medium-Sized Vestibular Schwannoma: The V-REX Randomized Clinical Trial
Abstract
Importance: Current guidelines for treating small- to medium-sized vestibular schwannoma recommend either upfront radiosurgery or waiting to treat until tumor growth has been detected radiographically.
Objective: To determine whether upfront radiosurgery provides superior tumor volume reduction to a wait-and-scan approach for small- to medium-sized vestibular schwannoma.
Design, setting, and participants: Randomized clinical trial of 100 patients with a newly diagnosed (<6 months) unilateral vestibular schwannoma and a maximal tumor diameter of less than 2 cm in the cerebellopontine angle as measured on magnetic resonance imaging. Participants were enrolled at the Norwegian National Unit for Vestibular Schwannoma from October 28, 2014, through October 3, 2017; 4-year follow-up ended on October 20, 2021.
Interventions: Participants were randomized to receive either upfront radiosurgery (n = 50) or to undergo a wait-and-scan protocol, for which treatment was given only upon radiographically documented tumor growth (n = 50). Participants underwent 5 annual study visits consisting of clinical assessment, radiological examination, audiovestibular tests, and questionnaires.
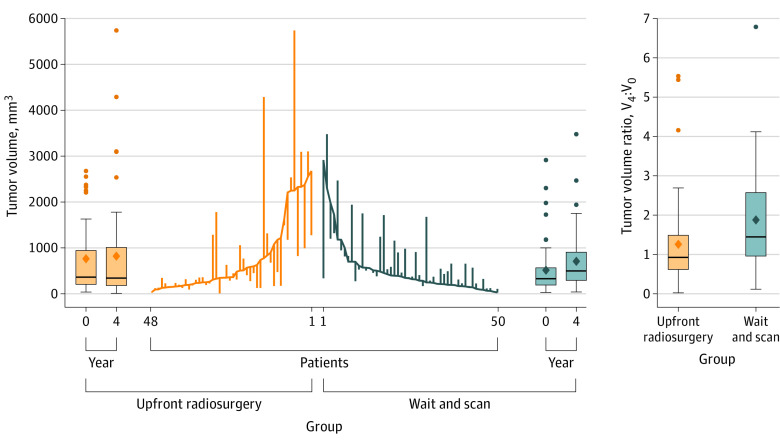
Main outcomes and measures: The primary outcome was the ratio between tumor volume at the trial end at 4 years and baseline (V4:V0). There were 26 prespecified secondary outcomes, including patient-reported symptoms, clinical examinations, audiovestibular tests, and quality-of-life outcomes. Safety outcomes were the risk of salvage microsurgery and radiation-associated complications.
Results: Of the 100 randomized patients, 98 completed the trial and were included in the primary analysis (mean age, 54 years; 42% female). In the upfront radiosurgery group, 1 participant (2%) received repeated radiosurgery upon tumor growth, 2 (4%) needed salvage microsurgery, and 45 (94%) had no additional treatment. In the wait-and-scan group, 21 patients (42%) received radiosurgery upon tumor growth, 1 (2%) underwent salvage microsurgery, and 28 (56%) remained untreated. For the primary outcome of the ratio of tumor volume at the trial end to baseline, the geometric mean V4:V0 was 0.87 (95% CI, 0.66-1.15) in the upfront radiosurgery group and 1.51 (95% CI, 1.23-1.84) in the wait-and-scan group, showing a significantly greater tumor volume reduction in patients treated with upfront radiosurgery (wait-and-scan to upfront radiosurgery ratio, 1.73; 95% CI, 1.23-2.44; P = .002). Of 26 secondary outcomes, 25 showed no significant difference. No radiation-associated complications were observed.
Conclusion and relevance: Among patients with newly diagnosed small- and medium-sized vestibular schwannoma, upfront radiosurgery demonstrated a significantly greater tumor volume reduction at 4 years than a wait-and-scan approach with treatment upon tumor growth. These findings may help inform treatment decisions for patients with vestibular schwannoma, and further investigation of long-term clinical outcomes is needed.
Trial registration: ClinicalTrials.gov Identifier: NCT02249572.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
