

Efficacy and Safety of Dapagliflozin in Patients With Chronic Kidney Disease Across the Spectrum of Frailty
- PMID: 37527836
- PMCID: PMC10809037
- DOI: 10.1093/gerona/glad181
Efficacy and Safety of Dapagliflozin in Patients With Chronic Kidney Disease Across the Spectrum of Frailty
Abstract
Background: A sizeable proportion of patients with chronic kidney disease (CKD) are reported to be frail. Here we examined the safety and efficacy of dapagliflozin in patients with CKD by frailty level.
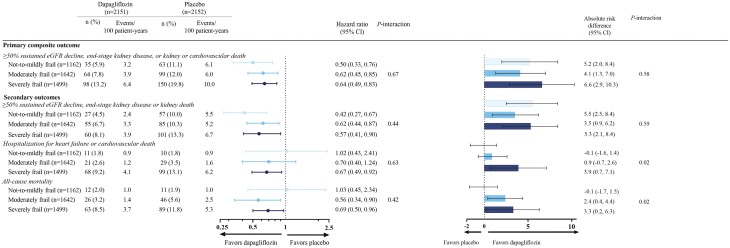
Methods: Adults with CKD, with/without type 2 diabetes, with an estimated glomerular filtration rate (eGFR) of 25-75 mL/min/1.73 m2, and urinary albumin-to-creatinine ratio 200-5 000 mg/g were randomized to dapagliflozin (10 mg/day) or placebo. The primary endpoint was a composite of sustained ≥50% eGFR decline, end-stage kidney disease (ESKD), or death from kidney or cardiovascular (CV) causes.
Results: Frailty index (FI), assessed by Rockwood cumulative deficit approach, was calculable in 4 303/4 304 (99.9%) patients: 1 162 (27.0%) in not-to-mildly frail (FI ≤0.210), 1 642 (38.2%) in moderately frail (FI 0.211-0.310), and 1 499 (34.8%) in severely frail categories (FI >0.311). Dapagliflozin reduced the risk of the primary composite endpoint across all FI categories (hazard ratios [95% confidence interval {CI}]: 0.50 [0.33-0.76], 0.62 [0.45-0.85], and 0.64 [0.49--0.83], respectively; p-interaction = 0.67). Results were similar for secondary outcomes including kidney composite outcome (sustained ≥50% eGFR decline, ESKD or death from kidney cause; p-interaction = 0.44), CV endpoint (heart failure hospitalization or CV death; p-interaction = 0.63), and all-cause mortality (p-interaction p = .42). Results were consistent when using FI as a continuous variable. Occurrence of serious adverse events was numerically lower in patients receiving dapagliflozin versus placebo in all FI categories (16.9% vs 20.1%, 26.3% vs 30.7%, and 42.9% vs 47.8%, in not-to-mildly, moderately, and severely frail categories, respectively).
Conclusions: The relative benefit of dapagliflozin for all outcomes was consistent across all frailty categories, with no difference in associated safety.
Keywords: Cardiovascular disease; Diabetes; SGLT-2 inhibitors.
© The Author(s) 2023. Published by Oxford University Press on behalf of The Gerontological Society of America.
Conflict of interest statement
P.V. report travel grants from AstraZeneca. N.J. report travel grants from AstraZeneca. J.H.B. reports receiving payment/honoraria from AstraZeneca, Bayer, and Novartis. He has served on a Data Safety Monitoring/Advisory Board for Bayer. M.S. reports receiving a grant for this manuscript, paid to his institution from AstraZeneca. He has also received travel grants from AstraZeneca and Novo Nordisk. G.M.C. has received fees from AstraZeneca for the DAPA-CKD trial steering committee. He serves on the Board of Directors for Satellite Healthcare, a nonprofit dialysis provider. He has received research grants from National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institute of Allergy and Infectious Diseases, and CSL Behring. He has served on trial steering committees with Akebia, AstraZeneca, Gilead, Sanifit, and Vertex. He has served as an advisor to Ardelyx, CloudCath, Durect, Miromatrix, Outset, Renibus, Reata, Sanifit, Unicycive, and Vertex. He has served on DSMBs for NIDDK, Bayer, Mineralys, and ReCor. D.C.W. has received consultancy fees and payment for travel and accommodation from AstraZeneca for this manuscript. He has received consultancy fees from Astellas, Boehringer Ingelheim, George Clinical, GlaxoSmithKline, Gilead, Merck Sharp and Dohme, ProKidney, Tricida, and Vifor. He also reports receiving payment/honoraria from Astellas, AstraZeneca, Boehringer Ingelheim, Intas, and Vifor. He had received a grant from the NIHR HTA program for the EVOLVE study and has received support for a leadership/fiduciary role from NIHR National specialty Lead for Renal Disorders (UK). R.P.-F. has received research grants from Fresenius Medical Care, National Council for Scientific and Technological Development, grants (paid to employer) from AstraZeneca, Boehringer‐Lilly, Novo Nordisk, Akebia, Bayer for participation in advisory Boards and educational activities. R.P.-F. is employed by Arbor Research Collaborative for health, who runs the DOPPS studies. A.M.L. is an employee and stockholder of AstraZeneca. R.C.-R. has support from AstraZeneca for this manuscript as being a member for the DAPA-CKD steering committee. He has received grants from AstraZeneca, GlaxoSmithKline, and Novo Nordisk; and honoraria as a speaker fees from fromAstraZeneca, Bayer, Boehringer Ingelheim, Amgen, and Janssen. He has received support for a leadership/fiduciary role from the Latin American Society of Nephrology as a member of the Diabetes Committee. P.R. has received honoraria to Steno Diabetes Center Copenhagen for steering group participation from AstraZeneca for this manuscript. He has received grants from AstraZeneca, Novo Nordisk, and Bayer; and consulting fees from Astellas, Astra Zeneca, Boehringer Ingelheim, Bayer, Gilead, Novo Nordisk, Merck, and Sanofi. He has also received honoraria/payment from EliLilly as speaker fees. J.J.V.M. has received payments from his employer, Glasgow University, as support on the current manuscript from AstraZeneca. He has received payment/honoraria for lecture fees from Abbott, Alkem Metabolics, Eris Lifesciences, Hikma, Lupin, Sun Pharmaceuticals, Medscape/Heart.Org, ProAdWise Communications, Radcliffe Cardiology, Servier, the Corpus. His institution has also received fees for his work on clinical trials, consulting and other activities from AstraZeneca, Cytokinetics, KBP Biosciences, Amgen, Bayer, Theracos, Ionis Pharmaceuticals, Dalcor Pharmaceuticals, Novartis, GlaxoSmithKline, Bristol-Myers Squibb, Boehringer Ingelheim, and Bayer. H.J.L.H. has received grants (paid to his institution [University Medical Center Groningen]) from AstraZeneca, Boehringer Ingelheim, Janssen, and Novo Nordisk. He has received consulting fees from AstraZeneca, Abbvie, Boehringer Ingelheim, CSL Behring, Bayer, Chinook, Dimerix, EliLilly, Gilead, Goldfinch, Merck, Novartis, NovoNordisk, Janssen, Travere Pharmaceuticals. He has received payment/honoraria from AstraZeneca and Novo Nordisk and travel grant from EliLilly.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
