

Risk of first-time major cardiovascular event among individuals with newly diagnosed type 2 diabetes: data from Danish registers
- PMID: 37528178
- PMCID: PMC10541344
- DOI: 10.1007/s00125-023-05977-6
Risk of first-time major cardiovascular event among individuals with newly diagnosed type 2 diabetes: data from Danish registers
Abstract
Aims/hypothesis: We aimed to examine whether individuals with initial omission of glucose-lowering drug treatment (GLDT), including those achieving initial remission of type 2 diabetes, may experience a higher risk of major adverse cardiovascular events (MACE) compared with well-controlled individuals on GLDT after a new type 2 diabetes diagnosis in real-world clinical practice. Furthermore, we examined whether a higher risk could be related to lower initiation of statins and renin-angiotensin system inhibitors (RASi).
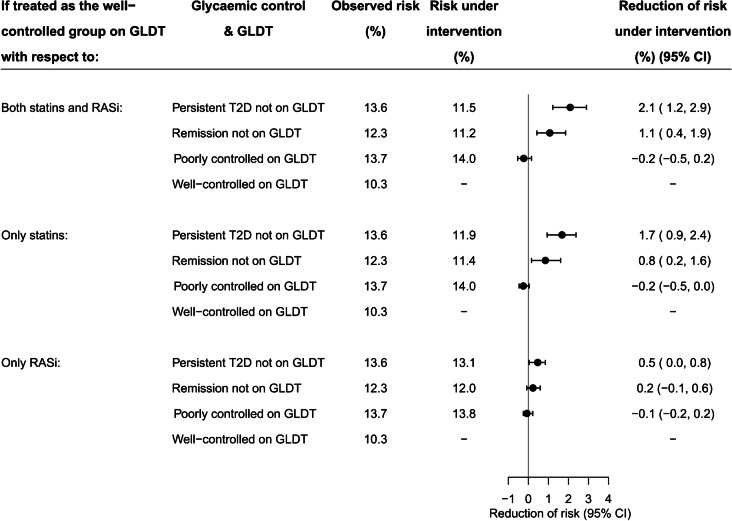
Methods: In this cohort study, we used Danish registers to identify individuals with a first measured HbA1c between 48 and 57 mmol/mol (6.5-7.4%) from 2014 to 2020. Six months later, we divided participants into four groups according to GLDT and achieved HbA1c (<48 vs ≥48 mmol/mol [6.5%]): well-controlled and poorly controlled on GLDT; remission and persistent type 2 diabetes not on GLDT. We reported how much the standardised 5 year risk of MACE could be reduced for each group if initiation of statins and RASi was the same as in the well-controlled group on GLDT.
Results: We included 14,221 individuals. Compared with well-controlled participants on GLDT, the 5 year standardised risk of MACE was higher in the three other exposure groups: by 3.3% (95% CI 1.6, 5.1) in the persistent type 2 diabetes group not on GLDT; 2.0% (95% CI 0.4, 3.7) in the remission group not on GLDT; and 3.5% (95% CI 1.3, 5.7) in the poorly controlled group on GLDT. Fewer individuals not on GLDT initiated statins and RASi compared with individuals on GLDT. If initiation of statins and RASi had been the same as in the well-controlled group on GLDT, participants not on GLDT could have reduced their risk of MACE by 2.1% (95% CI 1.2, 2.9) in the persistent type 2 diabetes group and by 1.1% (95% CI 0.4, 1.9) in the remission group.
Conclusions/interpretation: Compared with well-controlled individuals on GLDT, individuals not on initial GLDT had a higher 5 year risk of MACE, even among those achieving remission of type 2 diabetes. This may be related to lower use of statins and RASi.
Keywords: Cardiovascular disease; Glucose-lowering drug; Glycaemic control; Remission of type 2 diabetes; Renin–angiotensin system inhibitor; Statin; Type 2 diabetes.
© 2023. The Author(s).
Figures



References
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetologia. 2012;55:1577–1596. doi: 10.1007/s00125-012-2534-0. - DOI - PubMed
-
- Danish Society for General Practice and Danish Endocrine Society (2014) Pharmacological treatment of type 2 diabetes - aims and algorithms 2014. Available from https://endocrinology.dk/PDF/FarmakologiskbehandlingDM2rev2014.pdf. Accessed 21 October 2022
-
- Danish Society for General Practice and Danish Endocrine Society (2018) Pharmacological treatment of type 2 diabetes - aims and algorithms 2018. Available from https://vejledninger.dsam.dk/media/files/4/guidelines-2018-final.pdf. Accessed 21 October 2022
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
