

Dimethyl Fumarate or Teriflunomide for Relapsing-Remitting Multiple Sclerosis: A Meta-analysis of Post-marketing Studies
- PMID: 37528262
- PMCID: PMC10480378
- DOI: 10.1007/s13311-023-01416-x
Dimethyl Fumarate or Teriflunomide for Relapsing-Remitting Multiple Sclerosis: A Meta-analysis of Post-marketing Studies
Abstract
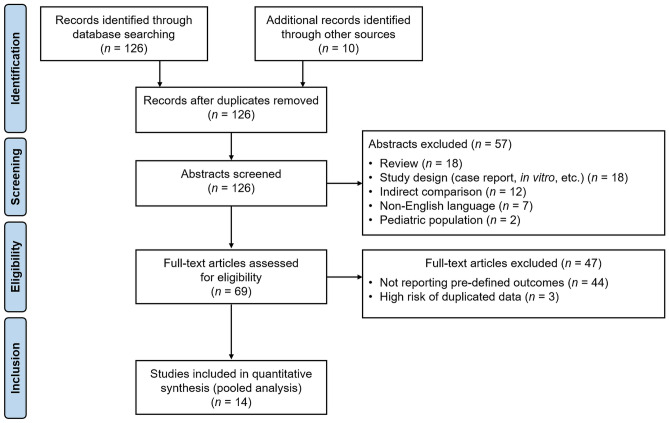
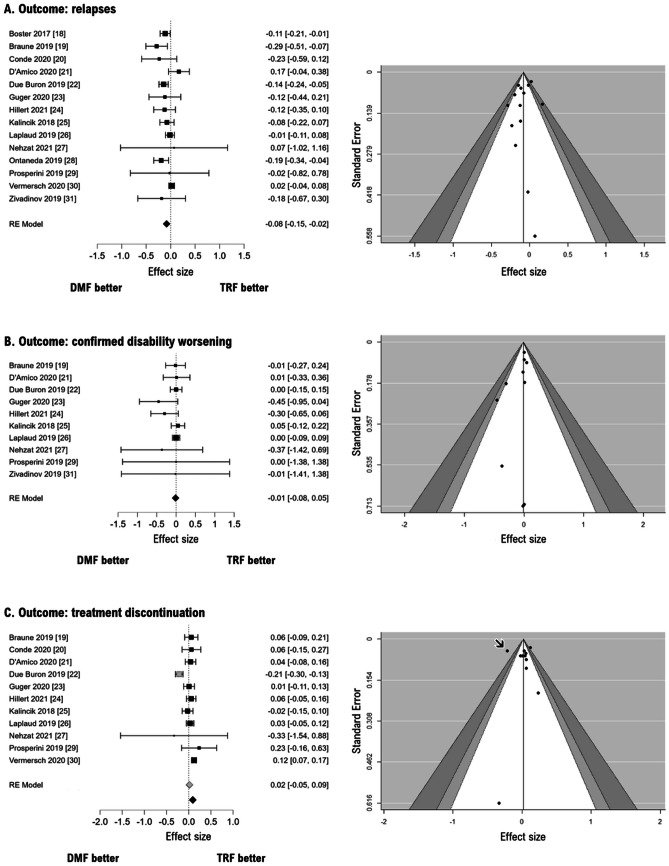
In the absence of head-to-head comparison trials, we aimed to compare the effectiveness of two largely prescribed oral platform disease-modifying treatments for relapsing-remitting multiple sclerosis, namely, dimethyl fumarate (DMF) and teriflunomide (TRF). We searched scientific databases to identify real-world studies reporting a direct comparison of DMF versus TRF. We fitted inverse-variance weighted meta-analyses with random effects models to estimate the risk ratio (RR) of relapse, confirmed disability worsening (CDW), and treatment discontinuation. Quantitative synthesis was accomplished on 14 articles yielding 11,889 and 8133 patients treated with DMF and TRF, respectively, with a follow-up ranging from 1 to 2.8 years. DMF was slightly more effective than TRF in reducing the short-term relapse risk (RR = 0.92, p = 0.01). Meta-regression analyses showed that such between-arm difference tends to fade in studies including younger patients and a higher proportion of treatment-naïve subjects. There was no difference between DMF and TRF on the short-term risk of CDW (RR = 0.99, p = 0.69). The risk of treatment discontinuation was similar across the two oral drugs (RR = 1.02, p = 0.63), but it became slightly higher with DMF than with TRF (RR = 1.07, p = 0.007) after removing one study with a potential publication bias that altered the final pooled result, as also confirmed by a leave-one-out sensitivity analysis. Discontinuation due to side effects and adverse events was reported more frequently with DMF than with TRF. Our findings suggest that DMF is associated with a lower risk of relapses than TRF, with more nuanced differences in younger naïve patients. On the other hand, TRF is associated with a lower risk of treatment discontinuation for side effects and adverse events.
Keywords: Dimethyl fumarate; Disease-modifying treatments; Head-to-head study; Multiple sclerosis; Teriflunomide.
© 2023. The American Society for Experimental Neurotherapeutics, Inc.
Conflict of interest statement
LP: consulting fees and/or speaker honoraria from Biogen, Celgene, Genzyme, Merck Serono, Novartis, and Teva; travel grants from Biogen, Genzyme, Novartis, and Teva; research grants from the Italian MS Society (Associazione Italiana Sclerosi Multipla) and Genzyme. CT: honoraria for speaking and travel grants from Biogen, Sanofi-Aventis, Merck Serono, Bayer-Schering, Teva, Genzyme, Almirall, and Novartis. SH: travel funding and/or speaker honoraria from Biogen, Roche, Genzyme, Novartis, CSL Behring. SR: personal fees and non-financial support from Biogen, Genzyme, Merck Serono, Novartis, and Teva. CG: fees as invited speaker or travel expenses for attending meeting from Biogen, Merck-Serono, Teva, Sanofi, Novartis, Genzyme.
Figures
References
-
- Mikol DD, Barkhof F, Chang P, et al. Comparison of subcutaneous interferon beta-1a with glatiramer acetate in patients with relapsing multiple sclerosis (the REbif vs glatiramer acetate in relapsing MS disease [REGARD] study): a multicentre, randomised, parallel, open-label trial. Lancet Neurol. 2008;7:903–914. doi: 10.1016/S1474-4422(08)70200-X. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
