

Incidence of hospital-acquired acute kidney injury and trajectories of glomerular filtration rate in older adults
- PMID: 37528401
- PMCID: PMC10394866
- DOI: 10.1186/s12882-023-03272-5
Incidence of hospital-acquired acute kidney injury and trajectories of glomerular filtration rate in older adults
Abstract
Background: In older adults, epidemiological data on incidence rates (IR) of hospital-acquired acute kidney injury (AKI) are scarce. Also, little is known about trajectories of kidney function before hospitalization with AKI.
Methods: We used data from biennial face-to-face study visits from the prospective Berlin Initiative Study (BIS) including community-dwelling participants aged 70+ with repeat estimated glomerular filtration rate (eGFR) based on serum creatinine and cystatin C. Primary outcome was first incident of hospital-acquired AKI assessed through linked insurance claims data. In a nested case-control study, kidney function decline prior to hospitalization with and without AKI was investigated using eGFR trajectories estimated with mixed-effects models adjusted for traditional cardiovascular comorbidities.
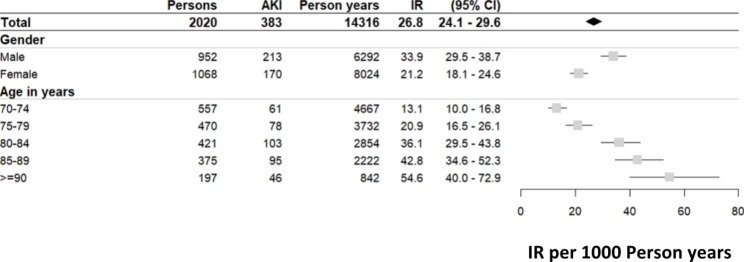
Results: Out of 2020 study participants (52.9% women; mean age 80.4 years) without prior AKI, 383 developed a first incident AKI, 1518 were hospitalized without AKI, and 119 were never hospitalized during a median follow-up of 8.8 years. IR per 1000 person years for hospital-acquired AKI was 26.8 (95% confidence interval (CI): 24.1-29.6); higher for men than women (33.9 (29.5-38.7) vs. 21.2 (18.1-24.6)). IR (CI) were lowest for persons aged 70-75 (13.1; 10.0-16.8) and highest for ≥ 90 years (54.6; 40.0-72.9). eGFR trajectories declined more steeply in men and women with AKI compared to men and women without AKI years before hospitalization. These differences in eGFR trajectories remained after adjustment for traditional comorbidities.
Conclusion: AKI is a frequent in-hospital complication in individuals aged 70 + showing a striking increase of IR with age. eGFR decline was steeper in elderly patients with AKI compared to elderly patients without AKI years prior to hospitalization emphasising the need for long-term kidney function monitoring pre-admission to improve risk stratification.
Keywords: AKI incidence; Acute kidney injury (AKI); Hospital-aquired AKI; In-hospital complication; Kidney function; Older adults; eGFR trajectories.
© 2023. The Author(s).
Conflict of interest statement
NE is member of an EAB for Bayer AG Leverkusen. ES has received grants from the National Kidney Foundation for editorial board (AJKD), consulting fees from Astra Zeneca, and honoraria for lectures from Akademie Niere, Berliner Dialyseseminar, Siemens Healthineers and Fresenius Kabi. MvdG has grant contracts from the Berlin Institute of Health and Novartis, received consulting fees from IEM, Pharvaris, Medtronic, Recor and Nephrolyx, honoraria from Bayer, Servier, Omron, Novartis, Boehringer, Recor, Medtrix, Streamedup, and participated in EAD for Novartis. MKK, AS, DH, AKF, NM, CL, YB, GB, and VW declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
