

Mouth breathing, dry air, and low water permeation promote inflammation, and activate neural pathways, by osmotic stresses acting on airway lining mucus
- PMID: 37529032
- PMCID: PMC10392678
- DOI: 10.1017/qrd.2023.1
Mouth breathing, dry air, and low water permeation promote inflammation, and activate neural pathways, by osmotic stresses acting on airway lining mucus
Abstract
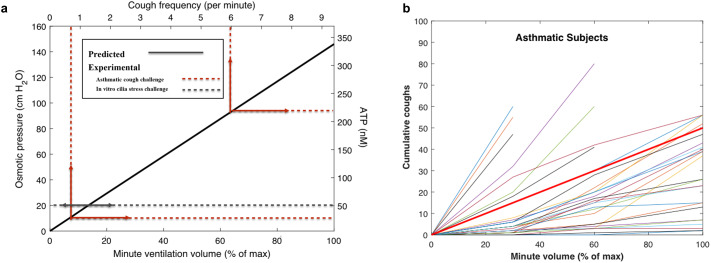
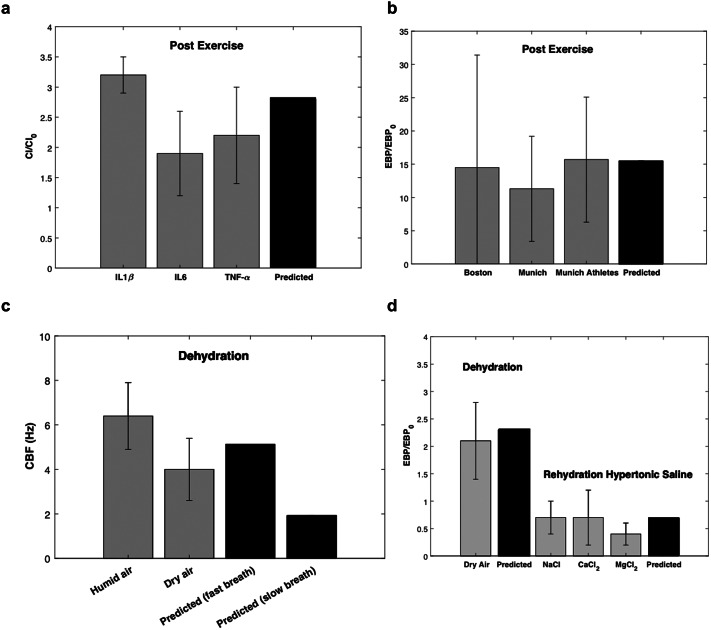
Respiratory disease and breathing abnormalities worsen with dehydration of the upper airways. We find that humidification of inhaled air occurs by evaporation of water over mucus lining the upper airways in such a way as to deliver an osmotic force on mucus, displacing it towards the epithelium. This displacement thins the periciliary layer of water beneath mucus while thickening topical water that is partially condensed from humid air on exhalation. With the rapid mouth breathing of dry air, this condensation layer, not previously reported while common to transpiring hydrogels in nature, can deliver an osmotic compressive force of up to around 100 cm H2O on underlying cilia, promoting adenosine triphosphate secretion and activating neural pathways. We derive expressions for the evolution of the thickness of the condensation layer, and its impact on cough frequency, inflammatory marker secretion, cilia beat frequency and respiratory droplet generation. We compare our predictions with human clinical data from multiple published sources and highlight the damaging impact of mouth breathing, dry, dirty air and high minute volume on upper airway function. We predict the hypertonic (or hypotonic) saline mass required to reduce (or amplify) dysfunction by restoration (or deterioration) of the structure of ciliated and condensation water layers in the upper airways and compare these predictions with published human clinical data. Preserving water balance in the upper airways appears critical in light of contemporary respiratory health challenges posed by the breathing of dirty and dry air.
Keywords: chronic cough; dehydration; hypertonic saline; mucus; respiratory droplets.
© The Author(s) 2023.
Conflict of interest statement
D.A.E. is a cofounder and shareholder of Sensory Cloud Inc. and a cofounder (while not a shareholder) of Pulmatrix. Each of these companies advances science, technology, and products for consumer health or therapeutic use by the inhalation of aerosols.
Figures
References
-
- Barbet JP, Chauveau M, Labbe S and Lockhart A (1988) Breathing dry air causes acute epithelial damage and inflammation of the Guinea pig trachea. Journal of Applied Physiology 64, 1851–1857. - PubMed
LinkOut - more resources
Full Text Sources