

The socioeconomic impact of disability progression in multiple sclerosis: A retrospective cohort study of the German NeuroTransData (NTD) registry
- PMID: 37529629
- PMCID: PMC10387702
- DOI: 10.1177/20552173231187810
The socioeconomic impact of disability progression in multiple sclerosis: A retrospective cohort study of the German NeuroTransData (NTD) registry
Abstract
Background: Multiple sclerosis (MS) is a progressively debilitating neurologic disease that poses significant costs to the healthcare system and workforce.
Objective: To evaluate the impact of MS disease progression on societal costs and quality of life (QoL) using data from the German NeuroTransData (NTD) MS registry.
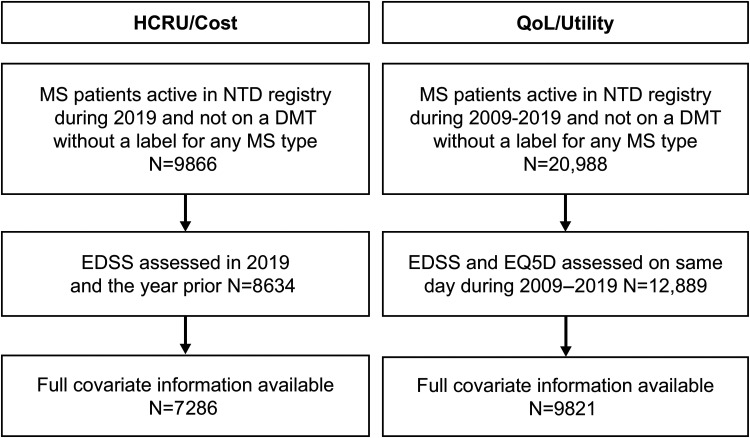
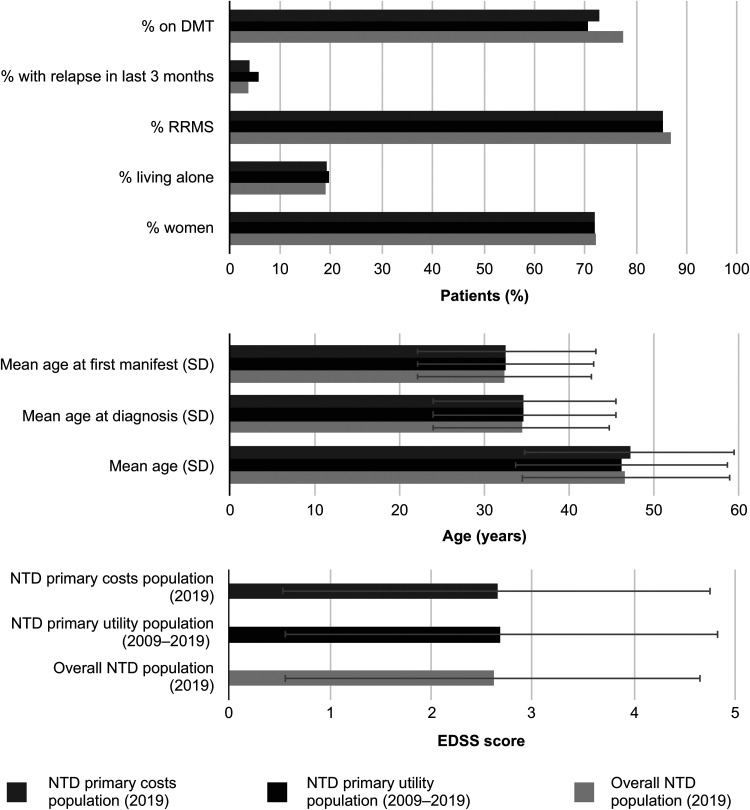
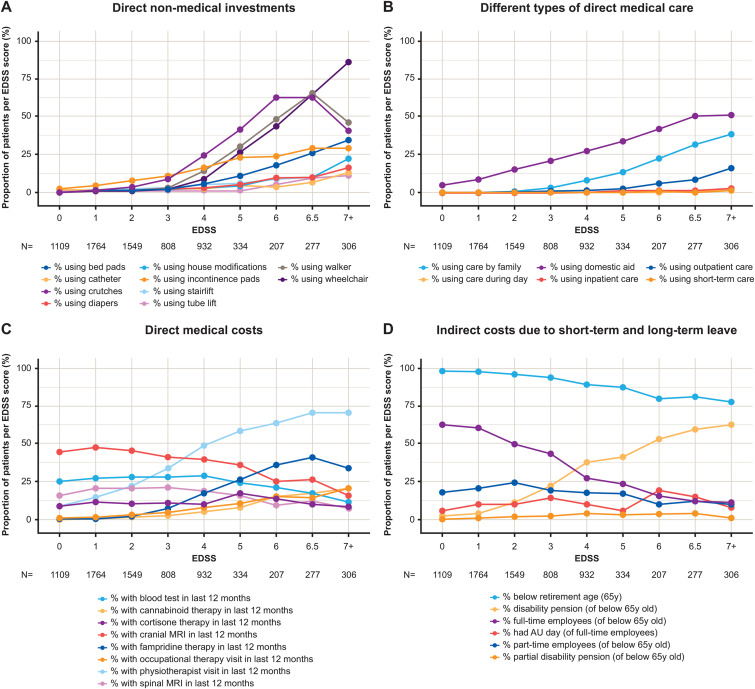
Methods: Cross-sectional cohort study. The cost cohort included patients with MS disability assessed using Expanded Disability Status Scale (EDSS) in 2019 while the QoL cohort included patients assessed using EDSS and EuroQol-5 Dimension 5-Levels between 2009 and 2019. Direct and indirect medical, and non-medical resource use was quantified and costs derived from public sources.
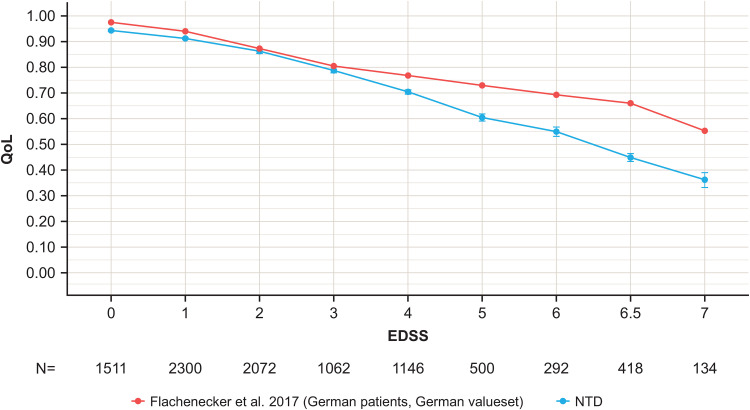
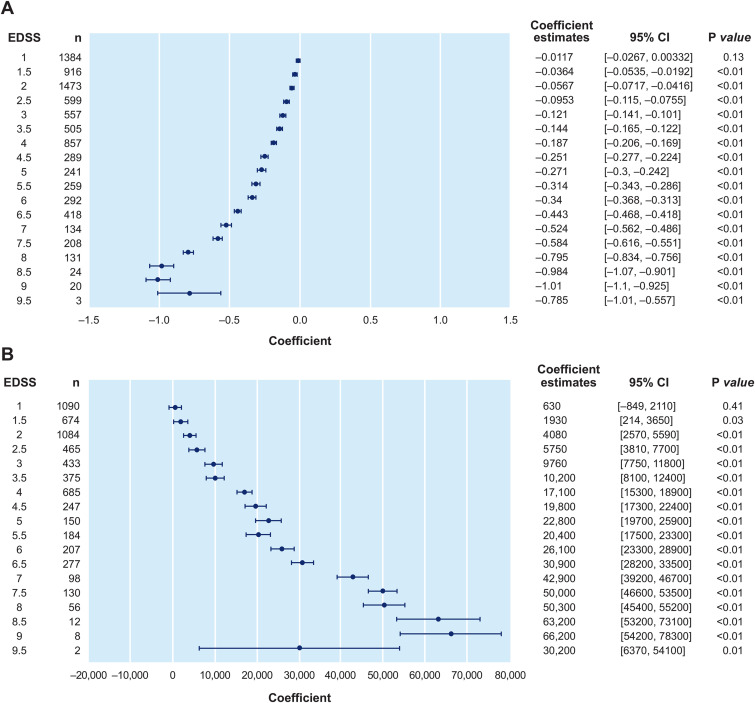
Results: Within the QoL cohort (n = 9821), QoL worsened with increasing EDSS. Within the cost cohort (n = 7286), increasing resource use with increasing EDSS was observed. Societal costs per patient, excluding or including disease-modifying therapies, increased from €5694 or €19,315 at EDSS 0 to 3.5 to €25,419 or €36,499 at EDSS 4 to 6.5, and €52,883 or €58,576 at EDSS 7 to 9.5. In multivariate modeling, each 0.5-step increase in EDSS was significantly associated with increasing costs, and worsening QoL.
Conclusion: This study confirms the major socioeconomic burden associated with MS disability progression. From a socioeconomic perspective, delaying disability progression may benefit patients and society.
Keywords: Multiple sclerosis; disease progression; economic burden of disease; quality of life.
© The Author(s), 2023.
Conflict of interest statement
Paul Dillon was an employee of F. Hoffmann-La Roche Ltd, Basel, Switzerland during completion of the work related to this manuscript and has shares/ownership of F. Hoffmann-La Roche Ltd. Yanic Heer was an employee of PricewaterhouseCoopers (PwC), Zurich, Switzerland during completion of the work related to this manuscript. Eleni Karamasioti was an employee of PricewaterhouseCoopers (PwC), Zurich, Switzerland during completion of the work related to this manuscript. Erwan Muros-Le Rouzic is an employee of and shareholder in F. Hoffmann-La Roche Ltd, Basel, Switzerland. Giuseppe Marcelli is an employee of F. Hoffmann-La Roche Ltd, Basel, Switzerland. Danilo Di Maio is an employee of F. Hoffmann-La Roche Ltd, Basel, Switzerland. Stefan Braune received honoraria from Kassenärztliche Vereinigung Bayerns and health maintenance organizations for patient care, and from Biogen, Merck, NeuroTransData, Novartis, and Roche for consulting, project management, clinical studies, and lectures; he also received honoraria and expense compensation as a board member of NeuroTransData. Gisela Kobelt is president of EHE International GmbHan and employee of European Health Economics, Mulhouse, France. Jürgen Wasem is a professor for health services management at University Duisburg-Essen, Germany. He has received an honorarium for consulting study concept and quality assurance of data calculations.
Figures
References
-
- The Multiple Sclerosis International Federation. Atlas of MS, atlasofms.org/map/germany/epidemiology/number-of-people-with-ms (2020, accessed 15 September 2022). - PMC - PubMed
-
- Compston A, Coles A. Multiple sclerosis. Lancet 2008; 372: 1502–1517. - PubMed
-
- Noseworthy JH, Lucchinetti C, Rodriguez M, et al. Multiple sclerosis. N Engl J Med 2000; 343: 938–952. - PubMed
-
- Karussis D. The diagnosis of multiple sclerosis and the various related demyelinating syndromes: a critical review. J Autoimmun 2014; 48-49: 134–142. - PubMed
-
- Trisolini MA, Wiener J, et al. Global economic impact of multiple sclerosis. https://www.msif.org/wp-content/uploads/2014/09/Global_economic_impact_o... (2010, accessed November 26, 2022).
LinkOut - more resources
Full Text Sources
