

EMPA-KIDNEY: expanding the range of kidney protection by SGLT2 inhibitors
- PMID: 37529652
- PMCID: PMC10387399
- DOI: 10.1093/ckj/sfad082
EMPA-KIDNEY: expanding the range of kidney protection by SGLT2 inhibitors
Abstract
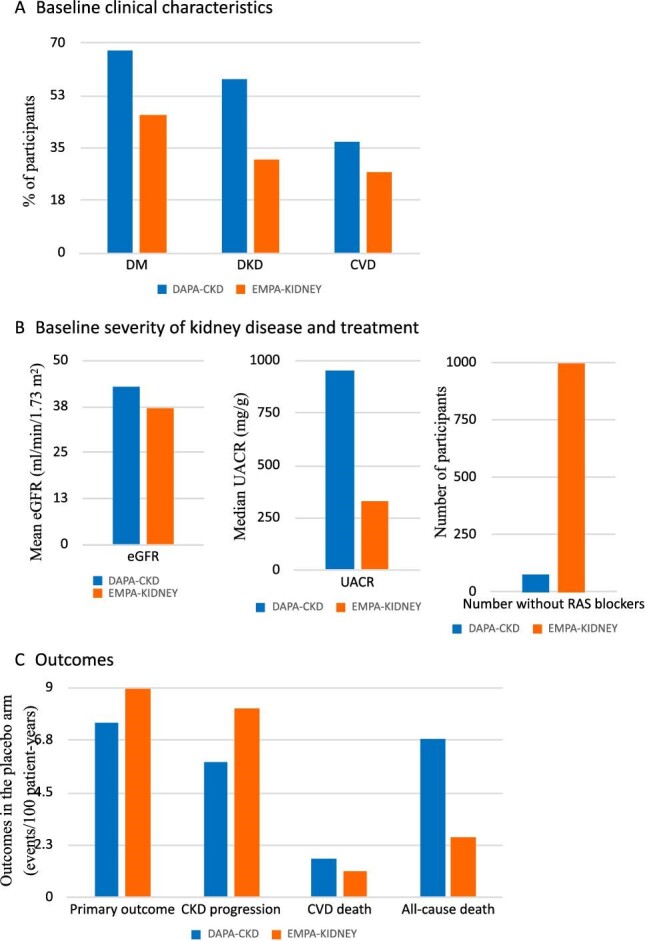
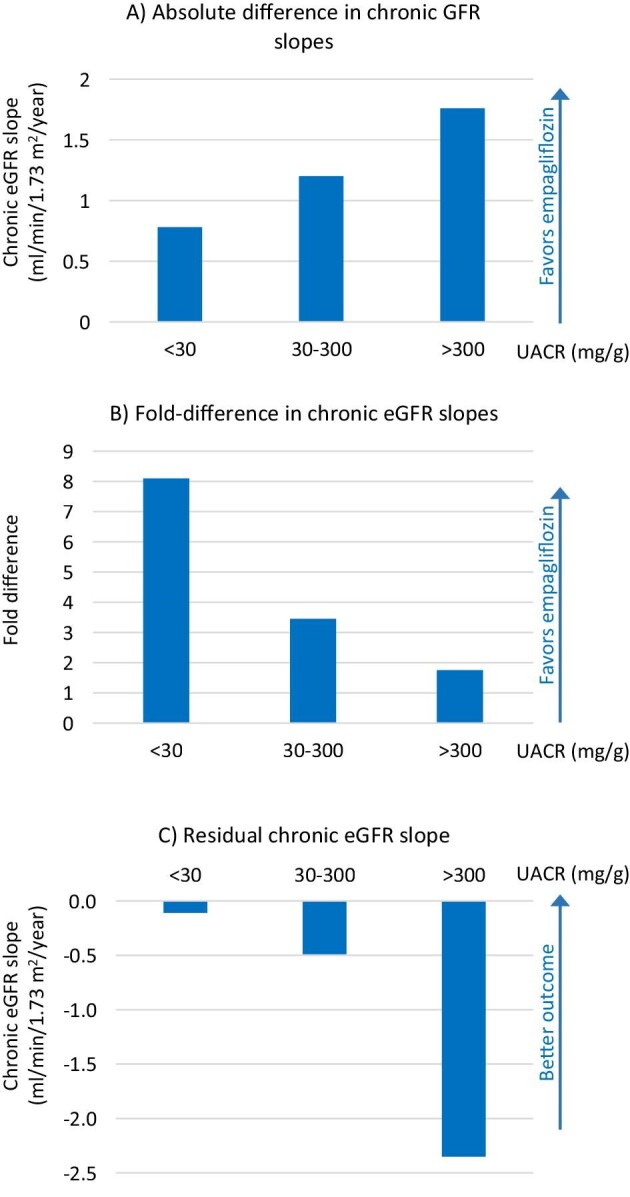
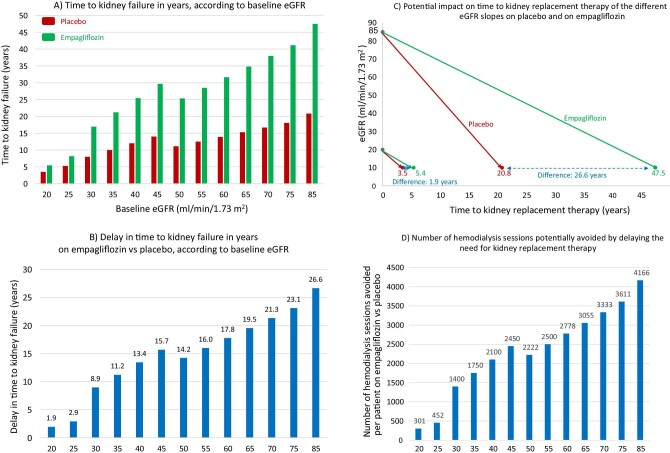
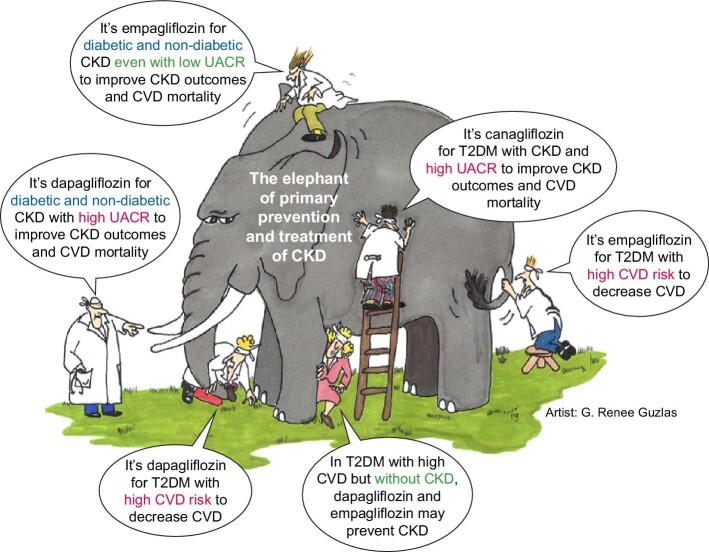
In the EMPA-KIDNEY (The Study of Heart and Kidney Protection With Empagliflozin) trial, empagliflozin reduced cardiorenal outcomes by 28% (hazard ratio 0.72; 95% confidence interval 0.64-0.82; P < .0001) in a diverse population of over 6000 chronic kidney disease (CKD) patients, of whom >50% were not diabetic. It expanded the spectrum of CKD that may benefit from sodium-glucose cotransporter 2 (SGLT2) inhibition to participants with urinary albumin: creatinine ratio <30 mg/g and estimated glomerular filtration rate (eGFR) >20 mL/min/1.73 m2 or even lower (254 participants had an eGFR 15-20 mL/min/1.73 m2). EMPA-KIDNEY was stopped prematurely because of efficacy, thus limiting the ability to confirm benefit on the primary outcome in every pre-specified subgroup, especially in those with more slowly progressive CKD. However, data on chronic eGFR slopes were consistent with benefit at any eGFR or urinary albumin:creatinine ratio level potentially delaying kidney replacement therapy by 2-27 years, depending on baseline eGFR. The representation of diverse causes of CKD (>1600 participants with glomerular disease, >1400 with hypertensive kidney disease, >450 with tubulointerstitial disease and >600 with unknown cause) was higher than in prior SGLT2 inhibitor trials, although polycystic kidney disease was excluded. Around 15% (almost 1000) of participants were not on renin-angiotensin system blockade. The clinical characteristics of the cohort differed from DAPA-CKD (A Study to Evaluate the Effect of Dapagliflozin on Renal Outcomes and Cardiovascular Mortality in Patients With Chronic Kidney Disease), as did the frequency of individual components of the primary outcome in the placebo arm. Thus, rather than compare EMPA-KIDNEY with DAPA-CKD, the results of both trials should be seen as complementary to those of other SGLT2 inhibitor trials. Overall, EMPA-KIDNEY, a recent meta-analysis and post hoc analyses of participants with type 2 diabetes mellitus (T2DM) but no baseline CKD in other trials, indicates that SGLT2 inhibitor treatment will benefit an expanded CKD population with diverse baseline albuminuria or eGFR values, presence of T2DM or cause of CKD, as well as providing primary prevention of CKD in at least the T2DM setting.
Keywords: RAS blockers; SGLT2 inhibitor; chronic kidney disease; normoalbuminuria; primary prevention; treatment.
© The Author(s) 2023. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
A.O. is one of the former Editors-in-Chief of Clinical Kidney Journal and has received grants from Sanofi and consultancy or speaker fees or travel support from Advicciene, Alexion, Astellas, Astrazeneca, Amicus, Amgen, Boehringer Ingelheim, Fresenius Medical Care, GSK, Bayer, Sanofi-Genzyme, Menarini, Mundipharma, Kyowa Kirin, Lilly, Freeline, Idorsia, Chiesi, Otsuka, Novo-Nordisk, Sysmex and Vifor Fresenius Medical Care Renal Pharma, and is Director of the CatedraMundipharma-UAM of diabetic kidney disease and the CatedraAstrazeneca-UAM of chronic kidney disease and electrolytes. He has stock in TelaraFarma. B.F.-F. has received grants from Esteve and consultancy or speaker fees or travel support from Astrazeneca, Bayer, Menarini, Novo-Nordisk Boehringer Ingelheim and Mundipharma. B.F.-F. is Editor for Nefroplus. P.S. has received consultancy fees from AstraZeneca, Bayer, HealThink, Innovis Pharma, PrimeView, Menarini and ReCor Medical; speaker fees from Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Genesis Pharma, Menarini, PeerVoice, Springer and Win Medica; research grants from AstraZeneca, Boehringer Ingelheim, Elpen and Servier. M.J.S. reports honorarium for conferences, consulting fees and advisory boards from AstraZeneca, NovoNordisk, Esteve, Vifor, Bayer, Mundipharma, Ingelheim Lilly, Jansen, ICU Medical, Travere Therapeutics, GE Healthcare and Boehringer. M.J.S is also the former Editor-in-Chief of Clinical Kidney Journal.
Figures
References
-
- Perez-Gomez MV, Bartsch L-A, Castillo-Rodriguez Eet al. . Clarifying the concept of chronic kidney disease for non-nephrologists. Clin Kidney J 2019;12:258–61. https://academic.oup.com/ckj/article/12/2/258/5320336. - PMC - PubMed
-
- Disease Kidney: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013;3:1–150.
-
- Ortiz A, Wanner C, Gansevoort Ret al. . Chronic kidney disease as cardiovascular risk factor in routine clinical practice: a position statement by the Council of the European Renal Association. Nephrol Dial Transplant 2023;38:527–31. https://pubmed.ncbi.nlm.nih.gov/36216362/. - PMC - PubMed
-
- Ortiz A, Roger M, Jiménez VMet al. . RICORS2040: the need for collaborative research in chronic kidney disease. Clin Kidney J 2021;15:372–87. https://pubmed.ncbi.nlm.nih.gov/35211298/. - PMC - PubMed
-
- Foreman KJ, Marquez N, Dolgert Aet al. . Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016–40 for 195 countries and territories. Lancet North Am Ed 2018;392:2052–90. 10.1016/S0140-6736(18)31694-5. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
