

Quantitative aortography for assessment of aortic regurgitation in the era of percutaneous aortic valve replacement
- PMID: 37529710
- PMCID: PMC10389707
- DOI: 10.3389/fcvm.2023.1161779
Quantitative aortography for assessment of aortic regurgitation in the era of percutaneous aortic valve replacement
Abstract
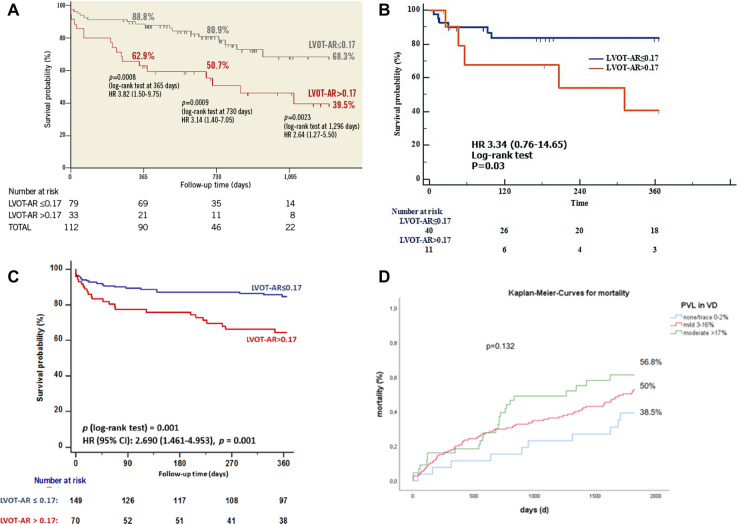
Paravalvular leak (PVL) is a shortcoming that can erode the clinical benefits of transcatheter valve replacement (TAVR) and therefore a readily applicable method (aortography) to quantitate PVL objectively and accurately in the interventional suite is appealing to all operators. The ratio between the areas of the time-density curves in the aorta and left ventricular outflow tract (LVOT-AR) defines the regurgitation fraction (RF). This technique has been validated in a mock circulation; a single injection in diastole was further tested in porcine and ovine models. In the clinical setting, LVOT-AR was compared with trans-thoracic and trans-oesophageal echocardiography and cardiac magnetic resonance imaging. LVOT-AR > 17% discriminates mild from moderate aortic regurgitation on echocardiography and confers a poor prognosis in multiple registries, and justifies balloon post-dilatation. The LVOT-AR differentiates the individual performances of many old and novel devices and is being used in ongoing randomized trials and registries.
Keywords: aortic regurgitation; paravalvular leak; quantitative aortography; transcatheter aortic valve implantation; transcatheter aortic valve replacement; videodensitometry.
© 2023 Abdelshafy, Serruys, Tsai, Revaiah, Grag, Aben, Schultz, Abdelghani, Tonino, Miyazaki, Rutten, Cox, Sahyoun, Teng, Tateishi, Abdel-Wahab, Piazza, Pighi, Modolo, van Mourik, Wykrzykowska, de Wintet, Lemos, de Brito, Kawashima, Søendergaard, Rosseel, Wang, Gao, Tao, Rück, Kim, van Royen, Terkelsen, Nissen, Adam, Rudolph, Wienemann, Torii, Neuman, Schoechlin, Chen, Elkoumy, Elzomor, Amat-Santos, Mylotte, Soliman and Onuma.
Conflict of interest statement
PWS reports personal fees from Philips/Volcano, SMT, Novartis, Xeltis, Merillife. PCR has no conflict of interest. Aben is an employee of Pie Medical Imaging. MC is employed by and holds shares of Xeltis BV CS is an employee of Philips Healthcare. MA-W reports other from Medtronic, other from Boston Scientific, outside the submitted work. NP is a consultant to Medtronic, Peijia, and MicroPort. RM is an employee of Boston Scientific. AR reports grants and personal fees from Boston Scientific, personal fees from Edwards Lifesciences, outside the submitted work. KK reports personal fees from Abbott, personal fees from Boston Scientific, personal fees from Edwards Lifesciences, personal fees from Medtronic, personal fees from Meril Life Sciences, outside the submitted work. NVR reports grants and personal fees from Abbott, grants from Philips, grants from Biotronik, and personal fees from Microport, outside the submitted work. Rudolph is a proctor, speaker’s honoraria of JenaValve. FJN reports personal fees from Amgen, personal fees from Boehringer Ingelheim, personal fees from Daiichi Sankyo, grants and personal fees from Pfizer, grants and personal fees from Biotronic, grants and personal fees from Edwards Lifesciences, grants from Medtronic, grants and personal fees from Bayer Healthcare, personal fees from Novartis, grants from GlaxoSmithKline, grants and personal fees from Boston Scientific, personal fees from Ferrer, outside the submitted work. IJA-S is a proctor for Medtronic, Boston Scientific and Meril Life. OS and YO report several institutional research grants, outside the submitted work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures










References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials