

Statistical plots in oncologic imaging, a primer for neuroradiologists
- PMID: 37529843
- PMCID: PMC11366205
- DOI: 10.1177/19714009231193158
Statistical plots in oncologic imaging, a primer for neuroradiologists
Abstract
The simplest approach to convey the results of scientific analysis, which can include complex comparisons, is typically through the use of visual items, including figures and plots. These statistical plots play a critical role in scientific studies, making data more accessible, engaging, and informative. A growing number of visual representations have been utilized recently to graphically display the results of oncologic imaging, including radiomic and radiogenomic studies. Here, we review the applications, distinct properties, benefits, and drawbacks of various statistical plots. Furthermore, we provide neuroradiologists with a comprehensive understanding of how to use these plots to effectively communicate analytical results based on imaging data.
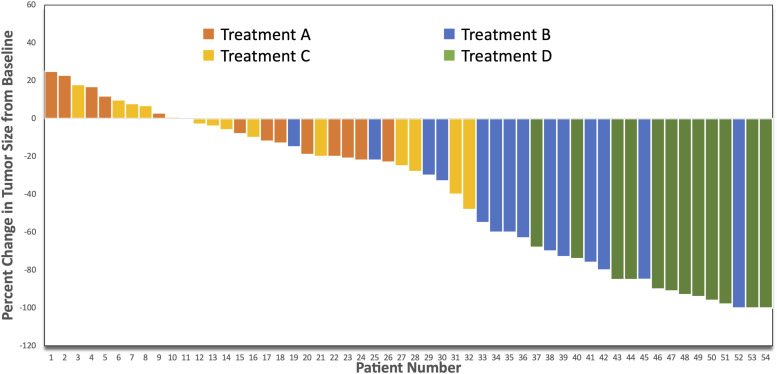
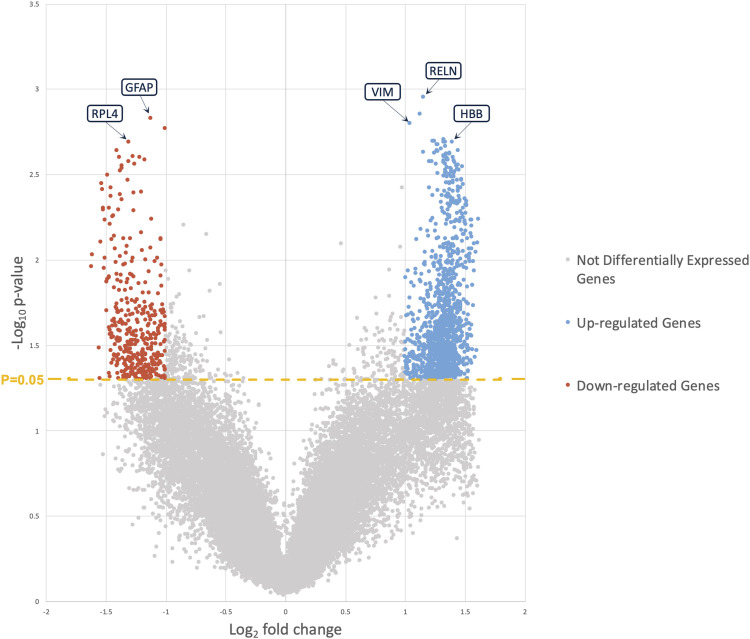
Keywords: Statistical plot; heatmap; principal component; spider plot; t-SNE; volcano plot; waterfall plot.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures















Similar articles
-
Short-Term Memory Impairment.2024 Jun 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Jun 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31424720 Free Books & Documents.
-
The Lived Experience of Autistic Adults in Employment: A Systematic Search and Synthesis.Autism Adulthood. 2024 Dec 2;6(4):495-509. doi: 10.1089/aut.2022.0114. eCollection 2024 Dec. Autism Adulthood. 2024. PMID: 40018061 Review.
-
Assessing the comparative effects of interventions in COPD: a tutorial on network meta-analysis for clinicians.Respir Res. 2024 Dec 21;25(1):438. doi: 10.1186/s12931-024-03056-x. Respir Res. 2024. PMID: 39709425 Free PMC article. Review.
-
Factors that impact on the use of mechanical ventilation weaning protocols in critically ill adults and children: a qualitative evidence-synthesis.Cochrane Database Syst Rev. 2016 Oct 4;10(10):CD011812. doi: 10.1002/14651858.CD011812.pub2. Cochrane Database Syst Rev. 2016. PMID: 27699783 Free PMC article.
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068
References
-
- Schriger DL, Sinha R, Schroter S. and et al. From submission to publication: a retrospective review of the tables and figures in a cohort of randomized controlled trials submitted to the British Medical Journal. Ann Emerg Med 2006; 48(6): 750–756. DOI: 10.1016/j.annemergmed.2006.06.017. - DOI - PubMed
-
- Tufte ER. The visual display of quantitative information. Graphics Press, 1983.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
