

Nivolumab for relapsed/refractory classical Hodgkin lymphoma: 5-year survival from the pivotal phase 2 CheckMate 205 study
- PMID: 37530622
- PMCID: PMC10589773
- DOI: 10.1182/bloodadvances.2023010334
Nivolumab for relapsed/refractory classical Hodgkin lymphoma: 5-year survival from the pivotal phase 2 CheckMate 205 study
Erratum in
-
Ansell SM, Bröckelmann PJ, von Keudell G, et al. Nivolumab for relapsed/refractory classical Hodgkin lymphoma: 5-year survival from the pivotal phase 2 CheckMate 205 study. Blood Adv. 2023;7(20):6266-6274.Blood Adv. 2024 Feb 27;8(4):829-831. doi: 10.1182/bloodadvances.2023012353. Blood Adv. 2024. PMID: 38353997 Free PMC article. No abstract available.
Abstract
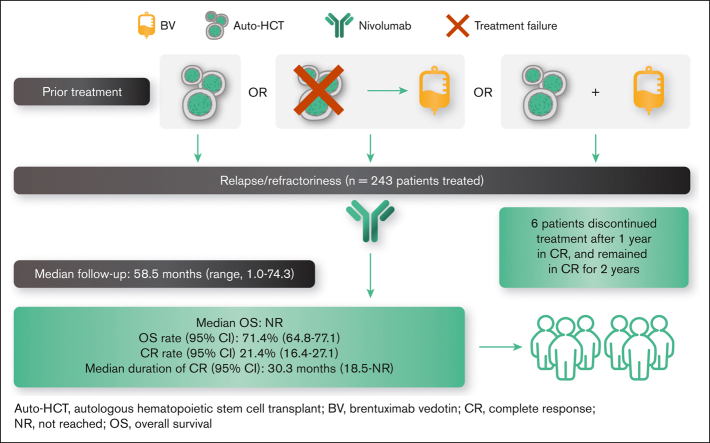
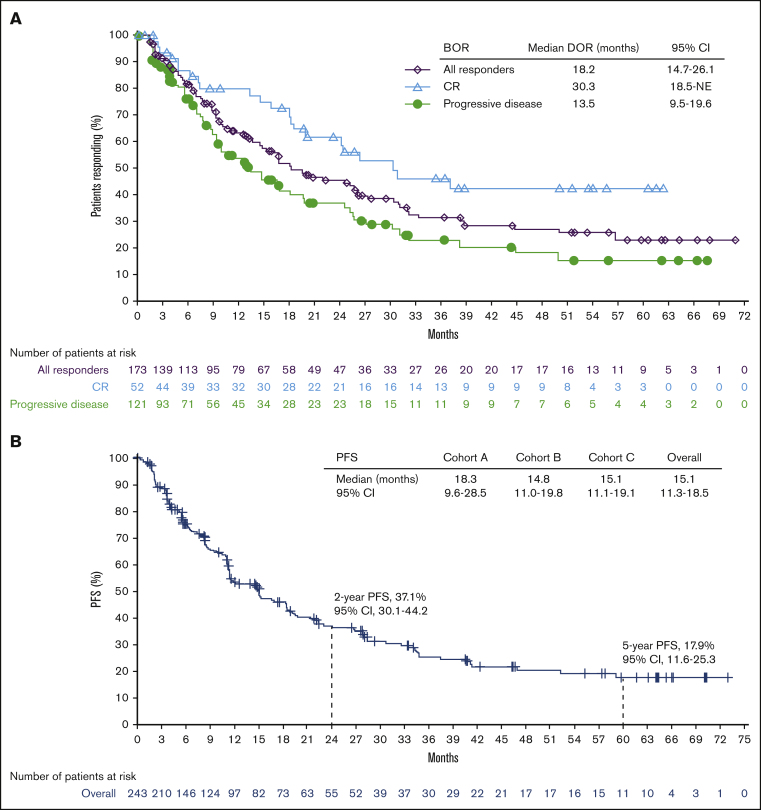
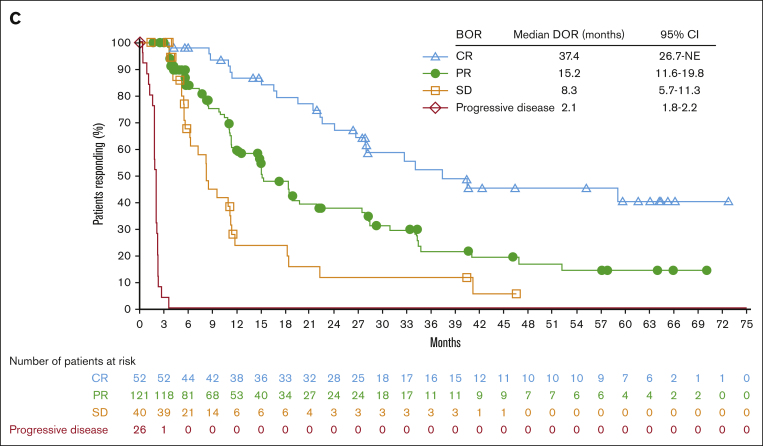
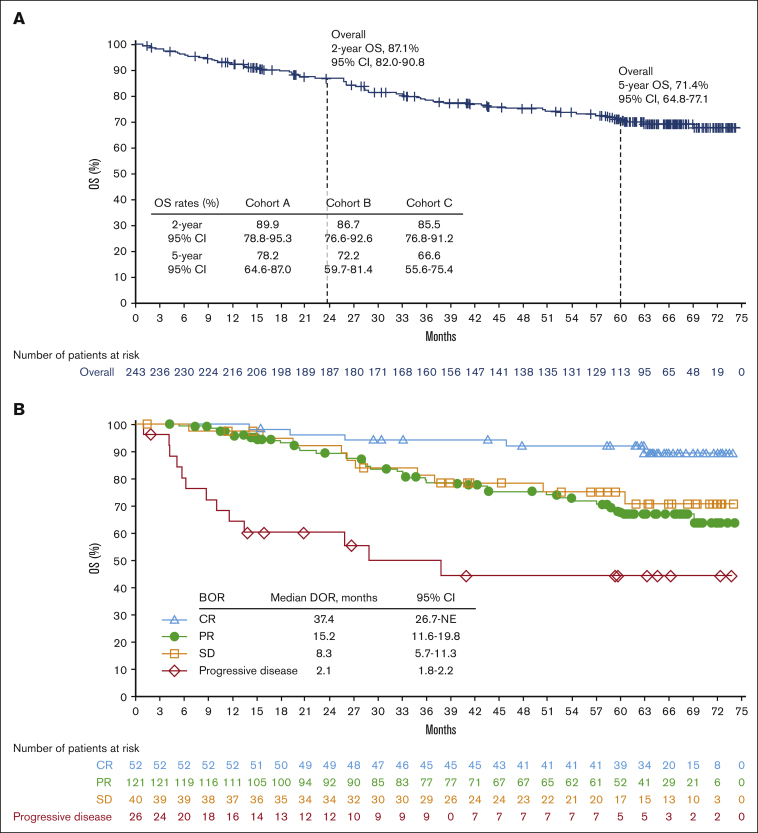
Patients with relapsed/refractory (R/R) classical Hodgkin lymphoma (cHL) for whom autologous hematopoietic cell transplantation (auto-HCT) had failed experienced frequent and durable responses to nivolumab in the phase 2 CheckMate 205 trial. We present updated results (median follow-up, ∼5 years). Patients with R/R cHL who were brentuximab vedotin (BV)-naive (cohort A), received BV after auto-HCT (cohort B), or received BV before and/or after auto-HCT (cohort C) were administered with nivolumab 3 mg/kg IV every 2 weeks until progression or unacceptable toxicity. Patients in cohort C with complete remission (CR) for 1 year could discontinue nivolumab and resume upon relapse. Among 243 patients (cohort A, n = 63; B, n = 80; and C, n = 100), the objective response rate (ORR) was 71.2% (95% confidence interval [CI], 65.1-76.8); the CR rate was 21.4% (95% CI, 16.4-27.1). Median duration of response, CR, and partial remission were 18.2 (95% CI, 14.7-26.1), 30.3, and 13.5 months, respectively. Median progression-free survival was 15.1 months (95% CI, 11.3-18.5). Median overall survival (OS) was not reached; OS at 5 years was 71.4% (95% CI, 64.8-77.1). In cohort C, all 3 patients who discontinued in CR and were subsequently re-treated achieved objective response. No new or unexpected safety signals were identified. This 5-year follow-up of CheckMate 205 demonstrated favorable OS and confirmed efficacy and safety of nivolumab in R/R cHL after auto-HCT failure. Results suggest patients may discontinue treatment after persistent CR and reinitiate upon progression. This trial was registered at www.clinicaltrials.gov as #NCT02181713.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: S.M.A. reports research support (institutional) from ADC Therapeutics, Bristol Myers Squibb, Regeneron, Seagen, Takeda, and Trillium. P.J.B. reports grants (institutional) from BeiGene, Bristol Myers Squibb, Merck Sharp and Dohme, and Takeda; consulting fees from Takeda; honoraria from BeiGene, Merck Sharp and Dohme, and Takeda; and travel/meeting support from Celgene. G.v.K. reports consulting fees from Merck. H.J.L. reports grants from Bristol Myers Squibb, Merck, Oncternal, Seagen, and Takeda; consulting fees from Century Therapeutics; and honoraria from Aptitude Health and the Korean Society of Cardio-oncology. A.S. reports consulting fees from Arquile, Incyte, and Sanofi; honoraria from AbbVie, Amgen, Arquile, AstraZeneca, Bayer, Bristol Myers Squibb, Celgene, Eisai, Eli Lilly, Gilead, Merck Sharp and Dohme, Novartis, Pfizer, Roche, Sandoz, Servier, and Takeda; and advisory board participation for Bayer, Bristol Myers Squibb, Eisai, Gilead, Merck Sharp and Dohme, Pfizer, and Servier. P.L.Z. reports honoraria from AstraZeneca, Bristol Myers Squibb, Gilead, Incyte, Kyowa Kirin, Merck, Novartis, Roche, Takeda, and Sanofi. G.P.C. reports research support from Amgen, AstraZeneca, Bristol Myers Squibb, and Pfizer; and honoraria from AbbVie, ADC Therapeutics, AstraZeneca, BeiGene, Gilead, Incyte, Kyowa Kirin, Novartis, Pfizer, Roche, SecuraBio, and Takeda. J.B.C. reports research support (institutional) from Bristol Myers Squibb/Celgene. J.K. reports research support (institutional) from AstraZeneca, Bristol Myers Squibb, and Merck; reports consulting fees from AbbVie, Antengene, Bristol Myers Squibb, Gilead, Karyopharm, Medison Ventures, Merck, Roche, and Seagen; reports honoraria from AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Gilead, Incyte, Janssen, Karyopharm, Merck, Novartis, Pfizer, Roche, and Seagen; and has chaired an advisory board for Lymphoma Canada. K.J.S. reports research support from Bristol Myers Squibb; consulting fees from Bristol Myers Squibb; research support (institutional) from Roche; honoraria from AbbVie, BeiGene, Bristol Myers Squibb, Janssen, Kyowa Kirin, Novartis, and Seagen; and advisory board participation for Regeneron. M.T. reports consulting fees and honoraria from AbbVie, AstraZeneca, Bristol Myers Squibb, Gilead, Janssen, MorphoSys, Novartis, Roche, and Takeda; and travel/meeting support from AstraZeneca, Gilead, Janssen, Roche, and Takeda. M.P. reports consulting fees from AstraZeneca, Bristol Myers Squibb, Merck Sharp and Dohme, and Roche; honoraria from Takeda and Thermo Fisher Scientific; and travel/meeting support from AstraZeneca, Merck Sharp and Dohme, and Roche. U.J. reports honoraria from Bristol Myers Squibb. W.W. is an employee of Syndena and reports research support from Amgen, AstraZeneca, Bristol Myers Squibb/Celgene, Bundesland Tirol Programm, European Commission, Janssen, Novartis, Roche, Sanofi, and Takeda; advisory board participation for Amgen, AbbVie, Bristol Myers Squibb/Celgene, EUSA Pharma, Fujimoto, Gilead, GlaxoSmithKline, Incyte, Janssen, Kite, Merck, Myelom- und Lymphomselbsthilfe Österreich, Novartis, Pfizer, Roche, Sandoz, Sanofi, and Takeda; and steering/safety committee participation for Amgen, Bristol Myers Squibb/Celgene, DSM, European Health Data & Evidence Network, Harmony, Honeur, and MorphoSys. J.M.-G. is an employee and holds stock in Bristol Myers Squibb. M.A.S. reports research support from AbbVie, AstraZeneca, Bayer, Bristol Myers Squibb, and Merck; and advisory board participation for AstraZeneca and Immunitas Therapeutics. A.E. reports consulting fees from AstraZeneca, Merck Sharp and Dohme, Takeda, and Tessa Pharma; grants from Bristol Myers Squibb; and honoraria from AstraZeneca, Hexal AG, Innovent, Janssen, Takeda, and TS Oncology. P.A. reports research funding from Kite; research funding (institutional) from Adaptive, Affimed, Bristol Myers Squibb, Genentech/Roche, IGM, Merck, Otsuka, Sigma Tau, and Tensha; honoraria from Bristol Myers Squibb and Merck; and consulting fees from Adaptive, ADC Therapeutics, Affimed, AstraZeneca, Bristol Myers Squibb, C4, Celgene, Daiichi Sankyo, Enterome, Epizyme, Genentech, GenMab, Infinity, Merck, Miltenyi, MorphoSys, Pfizer, Regeneron, Tessa, and Xencor. The remaining authors declare no competing financial interests.
The current affiliation for G.v.K. is Beth Israel Deaconess Medical Center/Harvard Medical School, Boston, MA.
Figures
References
-
- Crump M. Management of Hodgkin lymphoma in relapse after autologous stem cell transplant. Hematology Am Soc Hematol Educ Program. 2008;2008(1):326–333. - PubMed
-
- von Tresckow B, Müller H, Eichenauer DA, et al. Outcome and risk factors of patients with Hodgkin Lymphoma who relapse or progress after autologous stem cell transplant. Leuk Lymphoma. 2014;55(8):1922–1924. - PubMed
-
- Bartlett NL, Niedzwiecki D, Johnson JL, et al. Gemcitabine, vinorelbine, and pegylated liposomal doxorubicin (GVD), a salvage regimen in relapsed Hodgkin's lymphoma: CALGB 59804. Ann Oncol. 2007;18(6):1071–1079. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
