

Moderate-Intensity Statin With Ezetimibe Combination Therapy vs High-Intensity Statin Monotherapy in Patients at Very High Risk of Atherosclerotic Cardiovascular Disease: A Post Hoc Analysis From the RACING Randomized Clinical Trial
- PMID: 37531130
- PMCID: PMC10398545
- DOI: 10.1001/jamacardio.2023.2222
Moderate-Intensity Statin With Ezetimibe Combination Therapy vs High-Intensity Statin Monotherapy in Patients at Very High Risk of Atherosclerotic Cardiovascular Disease: A Post Hoc Analysis From the RACING Randomized Clinical Trial
Erratum in
-
Error in Figure.JAMA Cardiol. 2023 Sep 1;8(9):891. doi: 10.1001/jamacardio.2023.3311. JAMA Cardiol. 2023. PMID: 37702722 Free PMC article. No abstract available.
Abstract
Importance: High-intensity statin is strongly recommended in patients at very high risk (VHR) of atherosclerotic cardiovascular disease (ASCVD). However, concerns about statin-associated adverse effects result in underuse of this strategy in practice.
Objective: To evaluate the outcomes of a moderate-intensity statin with ezetimibe combination in VHR and non-VHR patients with ASCVD.
Design, setting, and participants: This was a post hoc analysis of the Randomized Comparison of Efficacy and Safety of Lipid Lowering With Statin Monotherapy vs Statin/Ezetimibe Combination for High-Risk Cardiovascular Disease (RACING) open-label, multicenter, randomized clinical trial. The study was conducted from February 2017 to December 2018 at 26 centers in Korea. Study participants included patients with documented ASCVD. Data were analyzed from April to June 2022.
Interventions: Patients were randomly assigned to moderate-intensity statin with ezetimibe (rosuvastatin, 10 mg, with ezetimibe, 10 mg) or high-intensity statin monotherapy (rosuvastatin, 20 mg). Patients at VHR for ASCVD were defined according to the 2018 American Heart Association/American College of Cardiology guidelines.
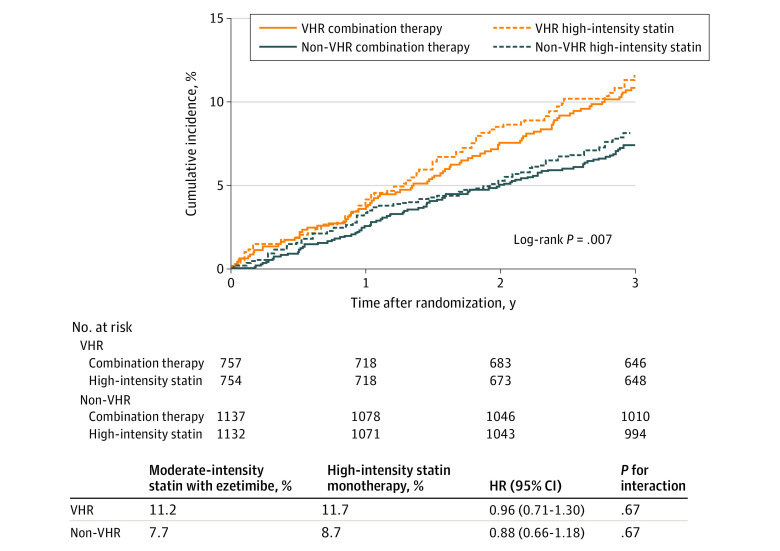
Main outcomes and measures: The primary end point was the 3-year outcome of cardiovascular death, coronary or peripheral revascularization, hospitalization of cardiovascular events, or nonfatal stroke.
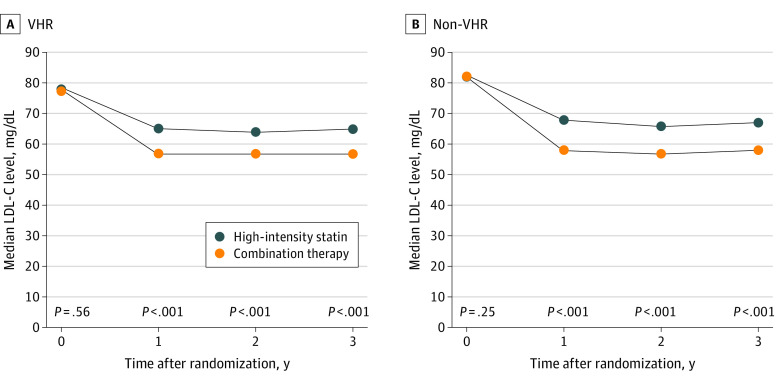
Results: A total of 3780 patients (mean [SD] age, 64 [10] years; 2826 male [75%]) in the RACING trial, 1511 (40.0%) were categorized as VHR, which was associated with a greater occurrence of the primary end point (hazard ratio [HR], 1.42; 95% CI, 1.15-1.75). There was no significant difference in the primary end point between those who received combination therapy and high-intensity statin monotherapy among patients with VHR disease (11.2% vs 11.7%; HR, 0.96; 95% CI, 0.71-1.30) and non-VHR disease (7.7% vs 8.7%; HR, 0.88; 95% CI, 0.66-1.18). The median low-density lipoprotein cholesterol (LDL-C) level was significantly lower in the combination therapy group than in the high-intensity statin group (VHR, 1 year: 57 [47-71] mg/dL vs 65 [53-78] mg/dL; non-VHR, 1 year: 58 mg/dL vs 68 mg/dL; P < .001). Furthermore, in both the VHR and non-VHR groups, combination therapy was associated with a significantly greater mean change in LDL-C level (VHR, 1 year: -19.1 mg/dL vs -10.1 mg/dL; 2 years: -22.3 mg/dL vs -13.0 mg/dL; 3 years: -18.8 mg/dL vs -9.7 mg/dL; non-VHR, 1 year: -23.7 mg/dL vs -12.5 mg/dL; 2 years: -25.2 mg/dL vs -15.1 mg/dL; 3 years: -23.5 mg/dL vs -12.6 mg/dL; all P < .001) and proportion of patients with LDL-C level less than 70 mg/dL (VHR, 1 year: 73% vs 58%; non-VHR, 1 year: 72% vs 53%; P < .001). Discontinuation or dose reduction of the lipid-lowering drug due to intolerance occurred less frequently in the combination therapy group (VHR, 4.6% vs 7.7%; P = .02; non-VHR, 5.0% vs 8.7%; P = .001).
Conclusions and relevance: Results suggest that the outcomes of ezetimibe combination observed in the RACING trial were consistent among patients at VHR of ASCVD.
Trial registration: ClinicalTrials.gov Identifier: NCT03044665.
Conflict of interest statement
Figures
References
-
- Grundy SM, Stone NJ, Bailey AL, et al. . 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;73(24):e285-e350. doi:10.1016/j.jacc.2018.11.003 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
