

Proregenerative extracellular matrix hydrogel mitigates pathological alterations of pelvic skeletal muscles after birth injury
- PMID: 37531414
- PMCID: PMC10460616
- DOI: 10.1126/scitranslmed.abj3138
Proregenerative extracellular matrix hydrogel mitigates pathological alterations of pelvic skeletal muscles after birth injury
Abstract
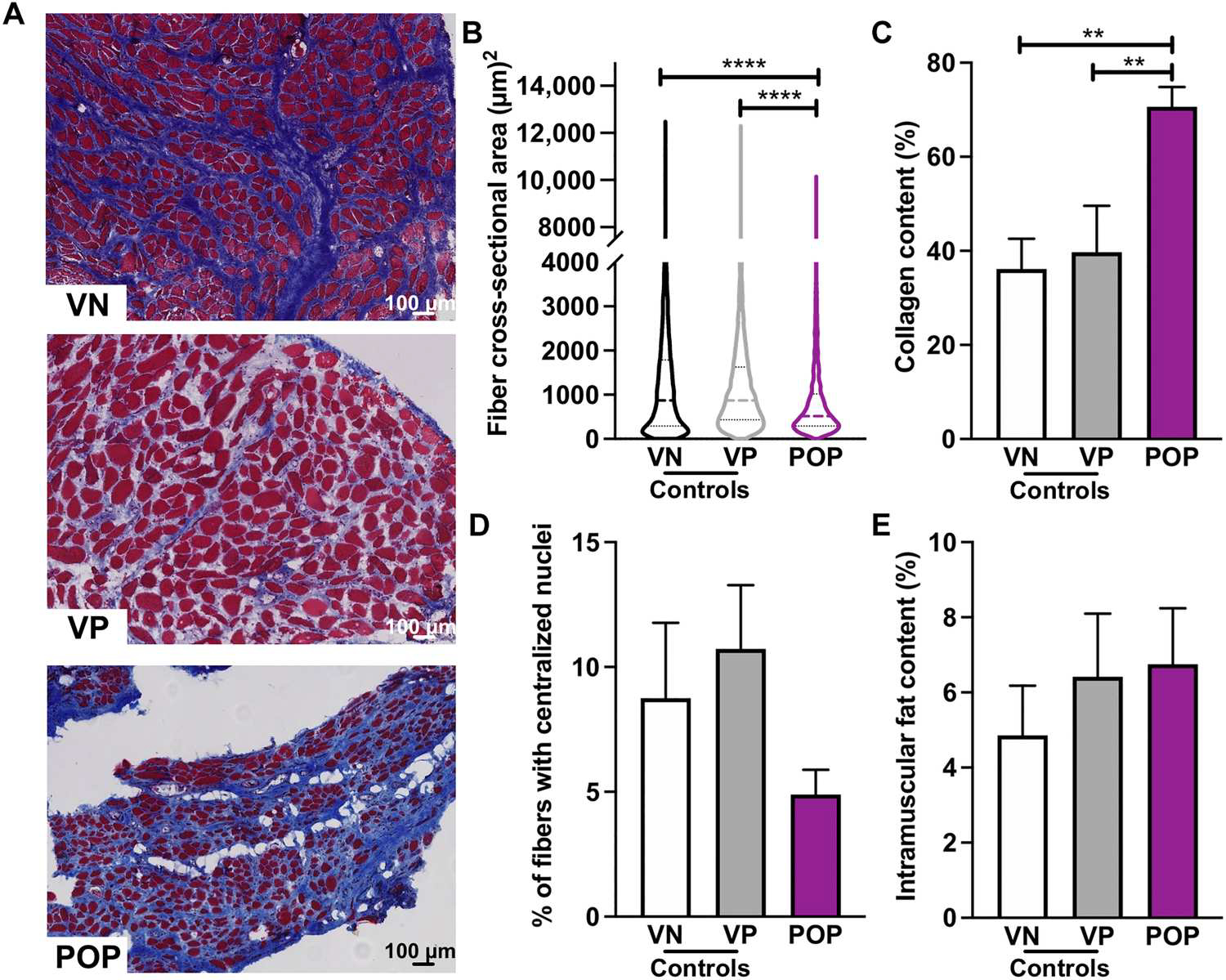
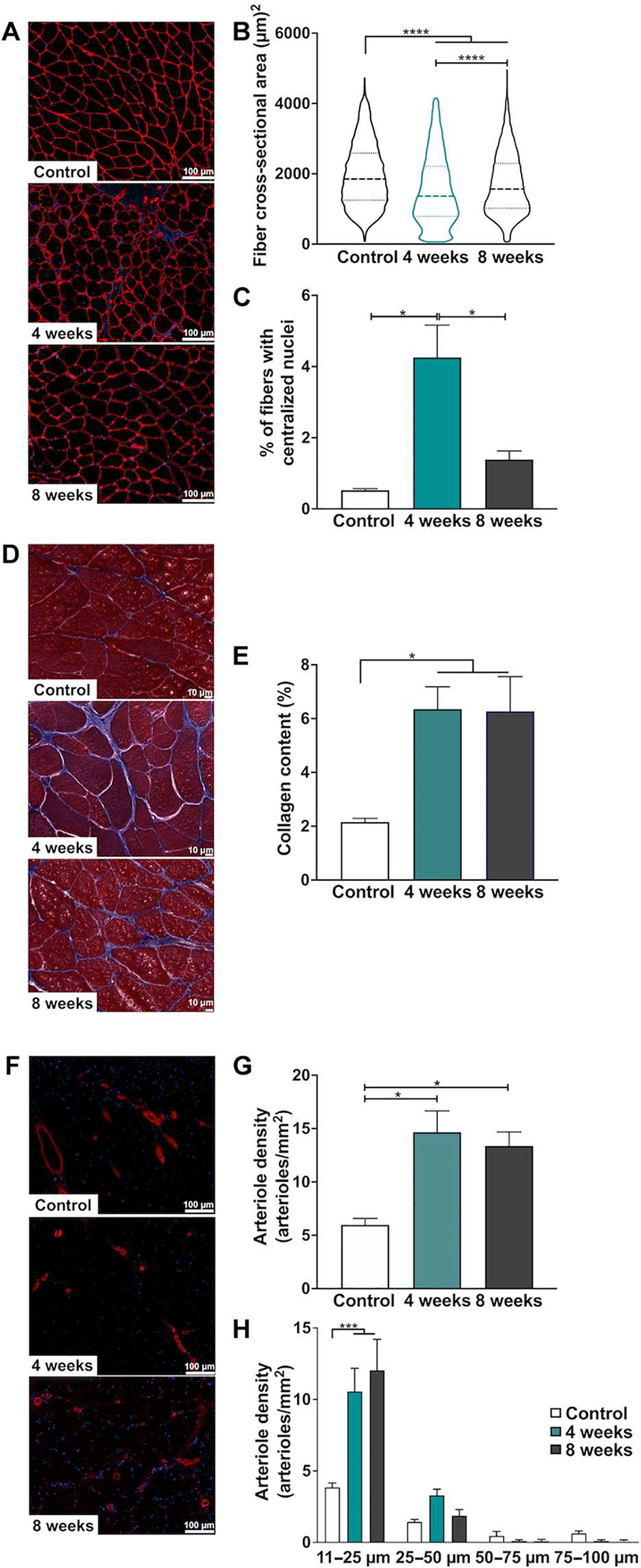
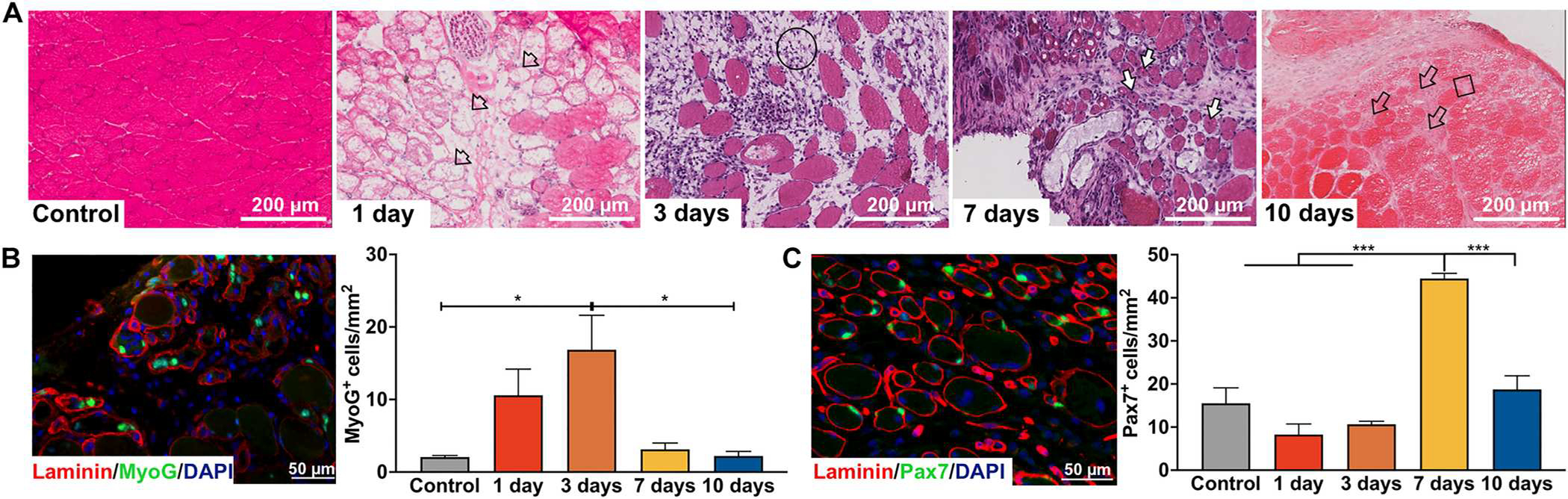
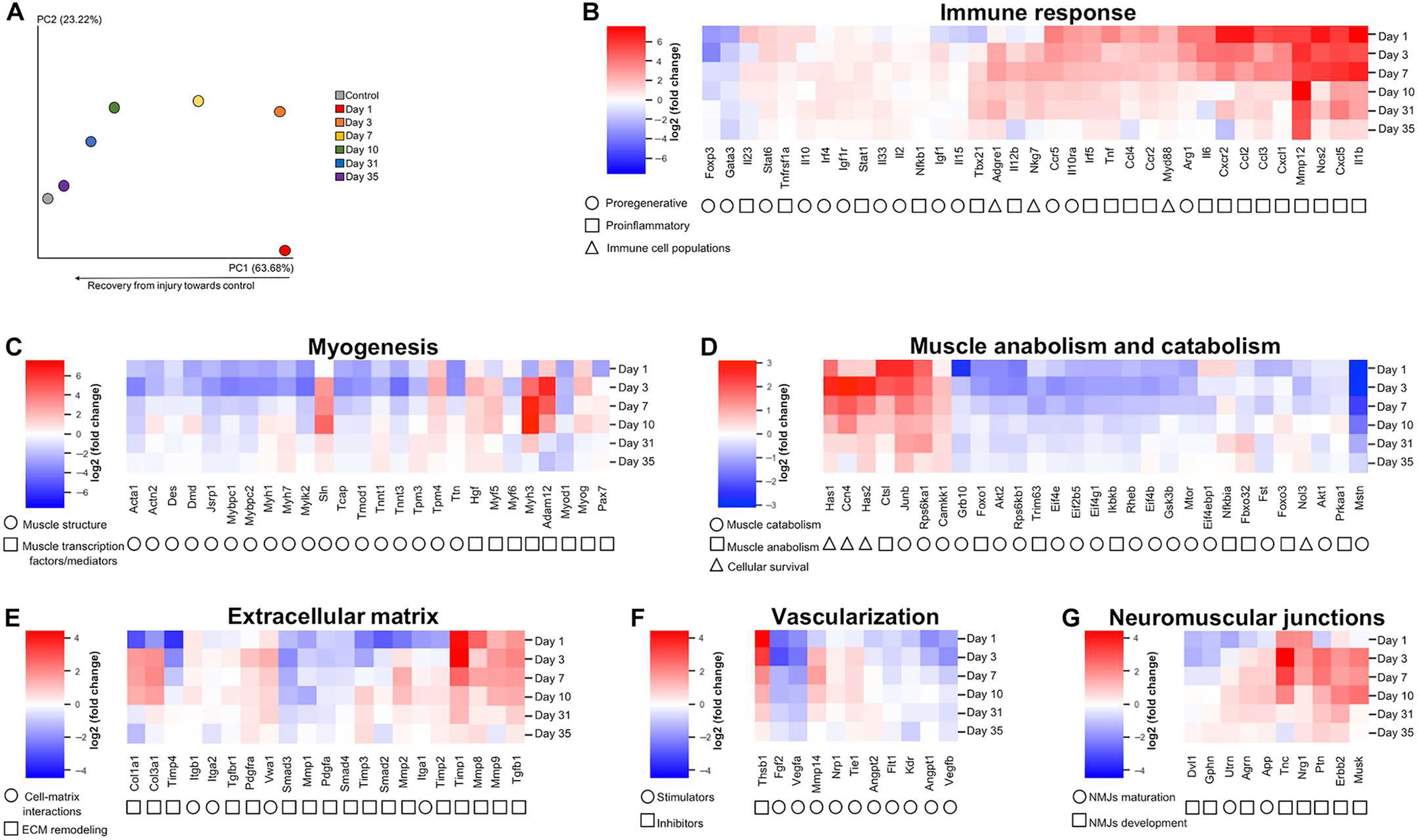
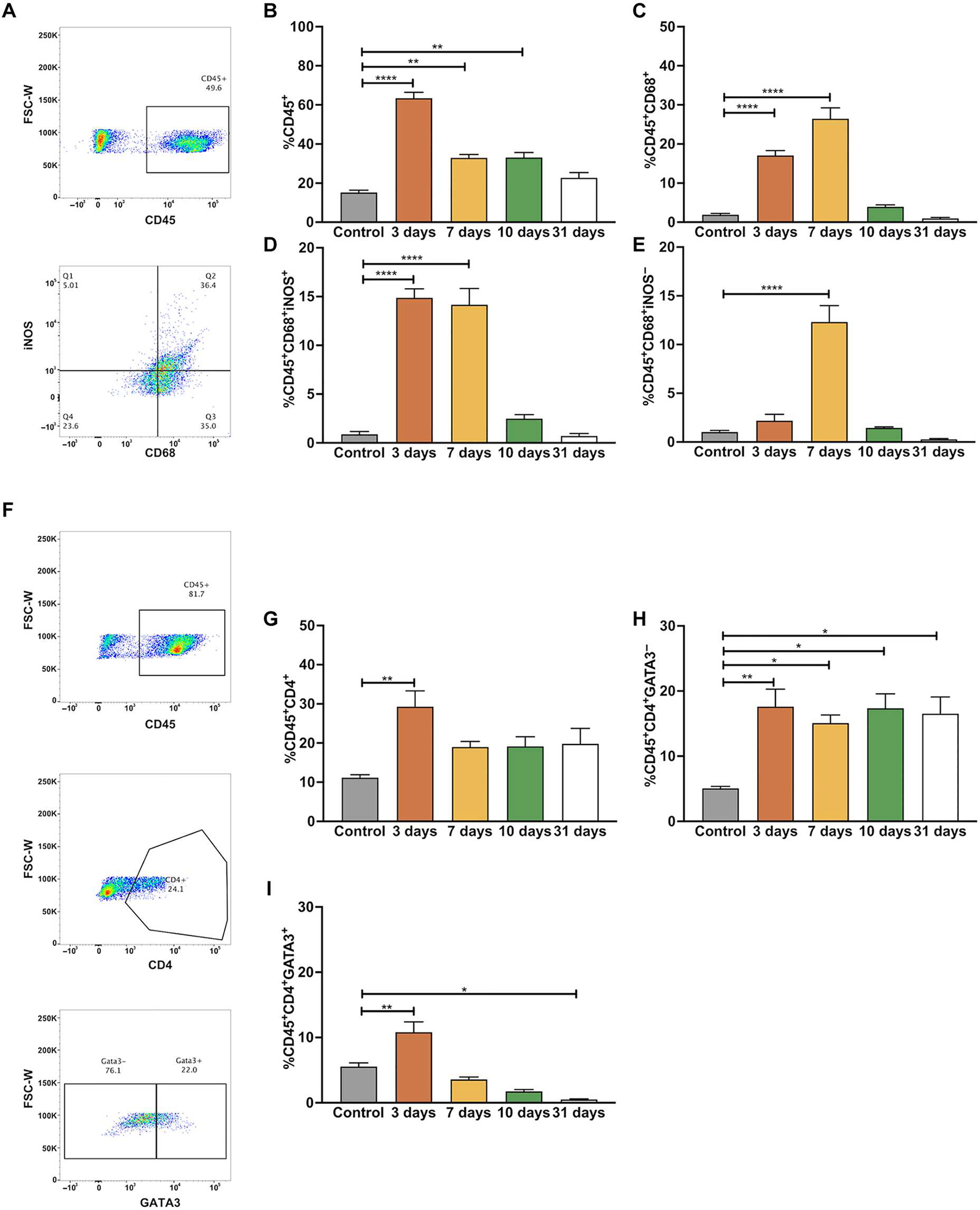
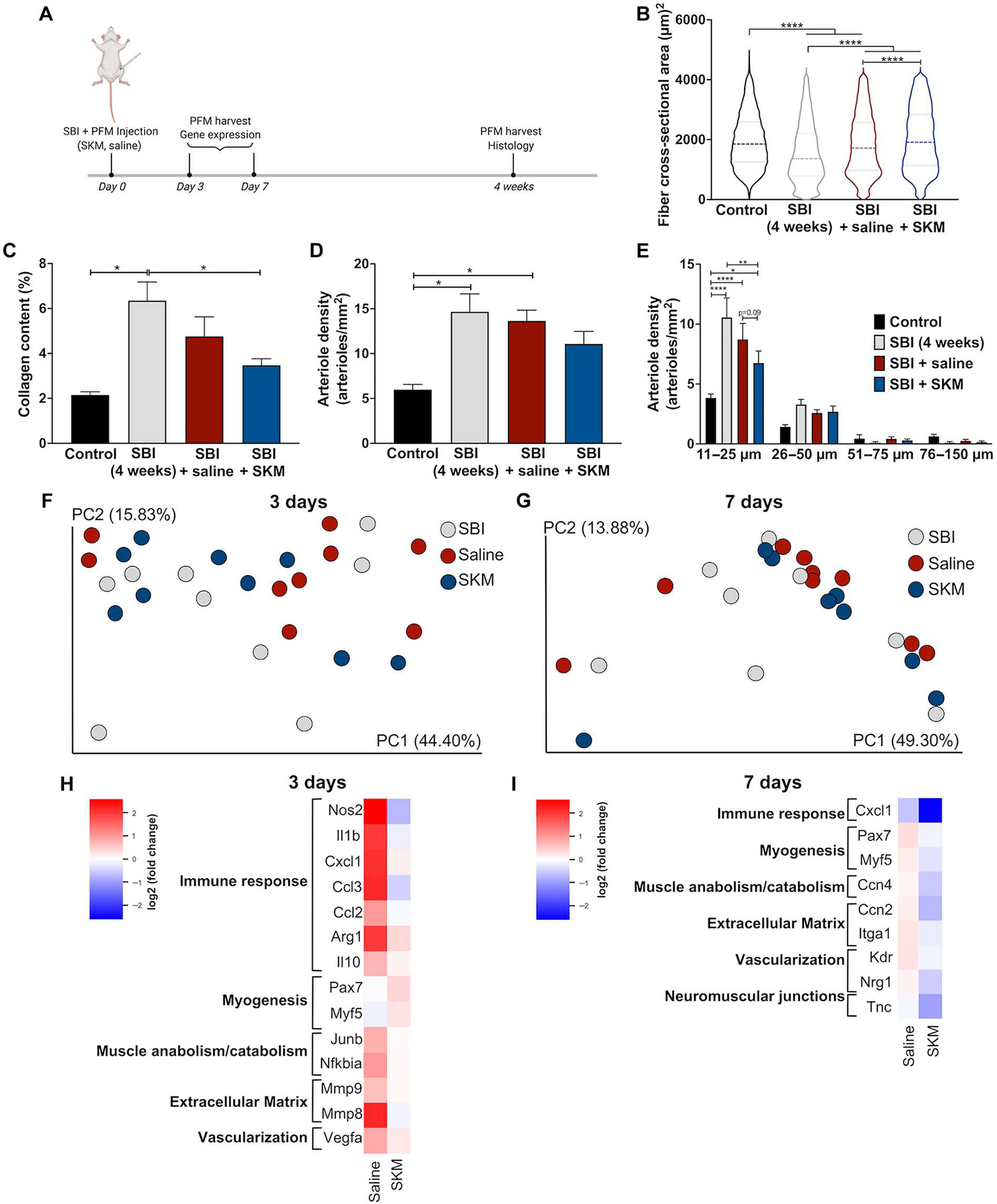
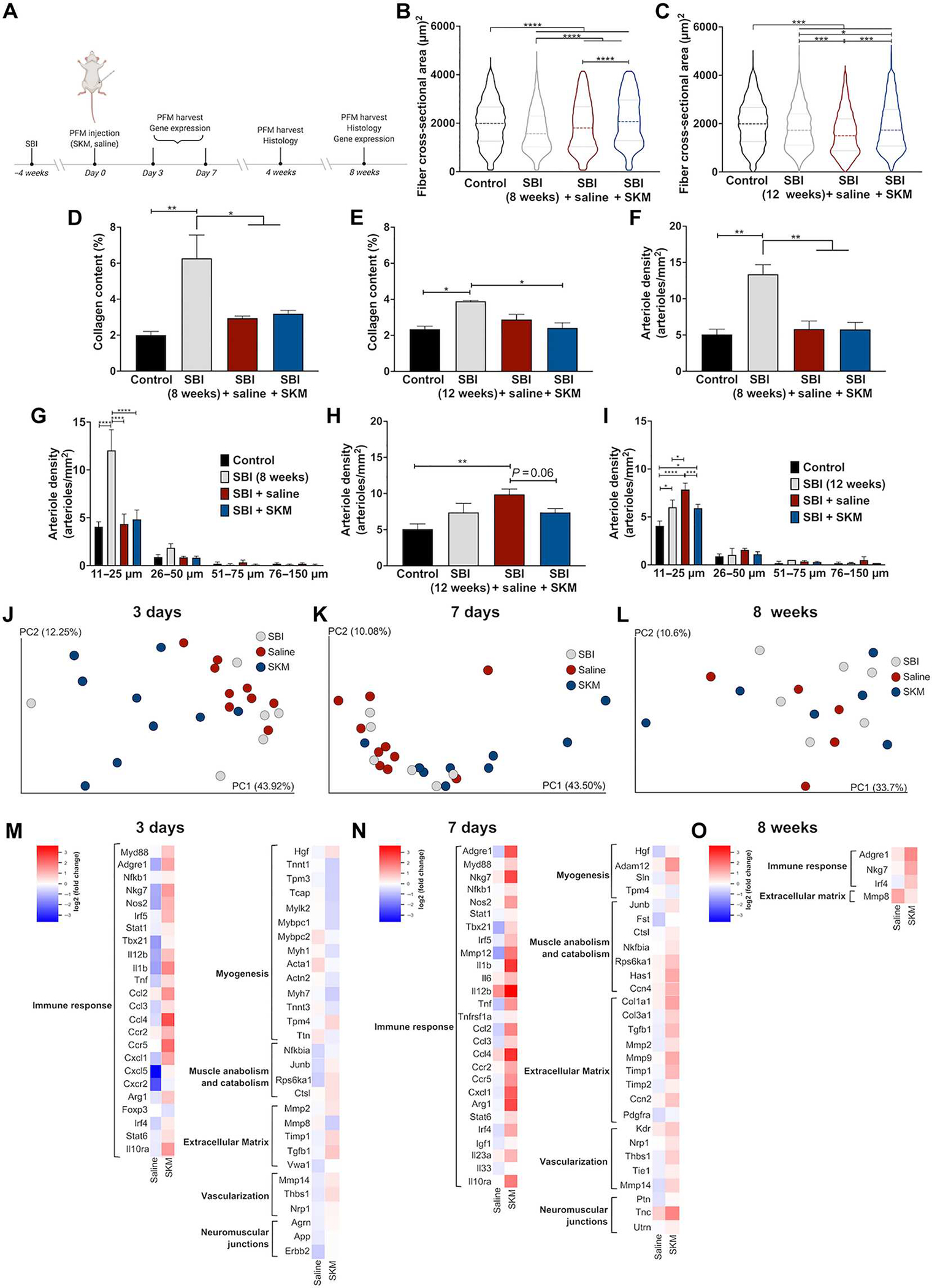
Pelvic floor disorders, including pelvic organ prolapse and urinary and fecal incontinence, affect millions of women globally and represent a major public health concern. Pelvic floor muscle (PFM) dysfunction has been identified as one of the leading risk factors for the development of these morbid conditions. Childbirth, specifically vaginal delivery, has been recognized as the most important potentially modifiable risk factor for PFM injury; however, the precise mechanisms of PFM dysfunction after parturition remain elusive. In this study, we demonstrated that PFMs exhibit atrophy and fibrosis in parous women with symptomatic pelvic organ prolapse. These pathological alterations were recapitulated in a preclinical rat model of simulated birth injury (SBI). The transcriptional signature of PFMs after injury demonstrated an impairment in muscle anabolism, persistent expression of genes that promote extracellular matrix (ECM) deposition, and a sustained inflammatory response. We also evaluated the administration of acellular injectable skeletal muscle ECM hydrogel for the prevention of these pathological alterations. Treatment of PFMs with the ECM hydrogel either at the time of birth injury or 4 weeks after injury mitigated PFM atrophy and fibrosis. By evaluating gene expression, we demonstrated that these changes are mainly driven by the hydrogel-induced enhancement of endogenous myogenesis, ECM remodeling, and modulation of the immune response. This work furthers our understanding of PFM birth injury and demonstrates proof of concept for future investigations of proregenerative biomaterial approaches for the treatment of injured pelvic soft tissues.
Conflict of interest statement
Figures
References
-
- Shen L, Yang J, Bai X, Sun Z, Analysis of the current status of pelvic floor dysfunction in urban women in Xi’an City. Ann. Palliat. Med. 9, 979–984 (2020). - PubMed
-
- Zeleke BM, Bell RJ, Billah B, Davis SR, Symptomatic pelvic floor disorders in community-dwelling older Australian women. Maturitas 85, 34–41 (2016). - PubMed
-
- Hasuda T, Ueda A, Wei C-N, Prevalence of symptomatic pelvic floor disorders among Japanese women. J. Women’s Health Care 6, 4 (2017).
-
- Blomquist JL, Carroll M, Munoz A, Handa VL, Pelvic floor muscle strength and the incidence of pelvic floor disorders after vaginal and cesarean delivery. Am. J. Obstet. Gynecol. 222, 62.e1–62.e8 (2020). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
