

Efficacy of azilsartan on left ventricular diastolic dysfunction compared with candesartan: J-TASTE randomized controlled trial
- PMID: 37532820
- PMCID: PMC10397297
- DOI: 10.1038/s41598-023-39779-y
Efficacy of azilsartan on left ventricular diastolic dysfunction compared with candesartan: J-TASTE randomized controlled trial
Abstract
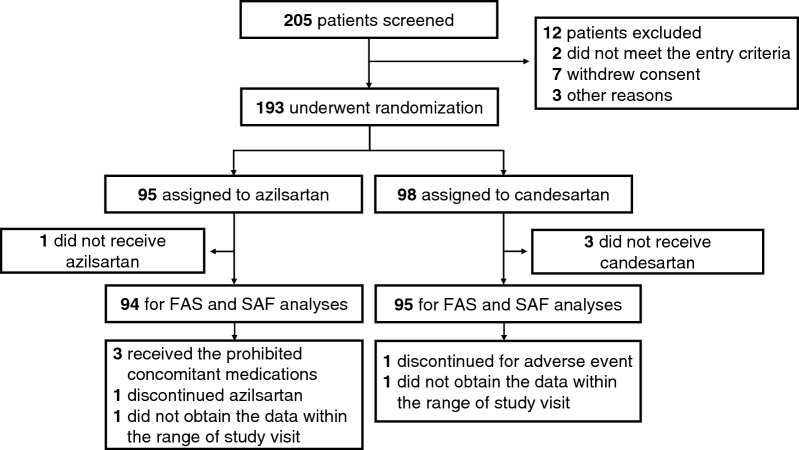
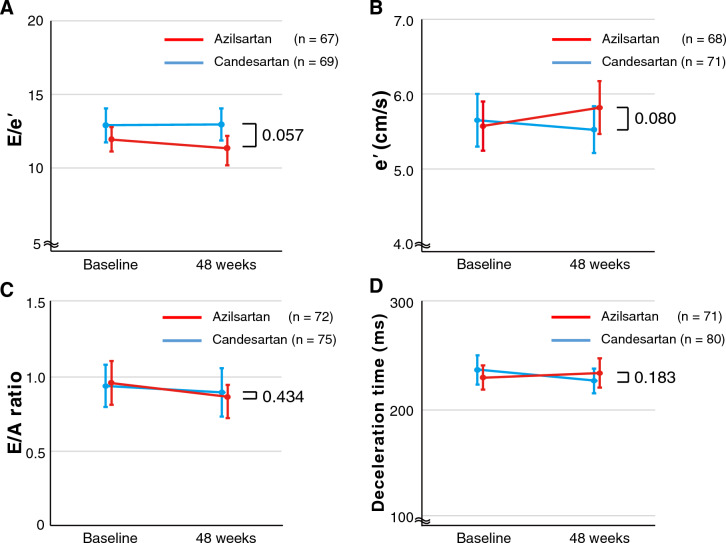
Characterized by ventricular and vascular stiffness, heart failure with preserved ejection fraction (HFpEF) has led to high morbidity and mortality. As azilsartan is an angiotensin receptor blocker with the highest myocardial and vascular affinities, azilsartan may improve the left ventricular (LV) diastolic function in patients with hypertension and either HFpEF or HF with mildly reduced ejection fraction (HFmrEF) more than candesartan. In this randomized, open-label trial, we randomly assigned 193 hypertensive patients with HF and LV ejection fraction ≥ 45% to 20 mg of azilsartan (n = 95) or 8 mg of candesartan (n = 98), once daily for 48 weeks. After the initiation of treatment, changes in the doses of the study drugs were permitted based on the patient's conditions, including blood pressure (median dose at 48 weeks: azilsartan 20.0 mg/day, candesartan 8.0 mg/day). The primary endpoint was the baseline-adjusted change in the ratio of peak early diastolic transmitral flow velocity (E) to early diastolic mitral annular velocity (e') (E/e'). Adjusted least-squares mean (LSM) change in E/e' was - 0.8 (95% confidence interval [CI] - 1.49 to - 0.04) in the azilsartan group and 0.2 (95% CI - 0.49 to 0.94) in the candesartan group, providing the LSM differences of - 1.0 (95% CI - 2.01 to 0.03, P = 0.057). The median change in left atrial volume index was - 2.7 mL/m2 with azilsartan vs 1.4 mL/m2 with candesartan (P = 0.091). The frequency of adverse events related to hypotension and hyperkalemia did not differ between the groups. The current study did not provide strong evidence that azilsartan improves LV diastolic dysfunction, and further confirmatory study is required.
© 2023. The Author(s).
Conflict of interest statement
YH, NI, YJL, K Matsuoka, S Matsuoka, HM, SN, T Sasaoka, S Takiuchi, and MY have nothing to disclose. SI reports a grant from Japan Society for the Promotion of Science, outside the submitted work. HT reports grants from the Japanese government, outside the submitted work. M Asakura reports personal fees from AstraZeneca, Ono, Otsuka, Novartis, Bayer, Daiichi Sankyo, Takeda, Pfizer, Boehringer Ingelheim, Mitsubishi Tanabe, Taisho, Kowa, Jansen, Nippon Shinyaku, and Astellas, outside the submitted work. YA reports grants from Japan Society for the Promotion of Science, grants from Japanese Agency for Medical Research and Development, grants from Japan Health Foundation, personal fees from AstraZeneca, personal fees from Novartis, personal fees from Daiichi Sankyo, personal fees from Otsuka, personal fees from Boehringer Ingelheim, personal fees from Ono, personal fees from Astellas, personal fees from Bayer, personal fees from Eli Lilly, and personal fees from Edwards Lifesciences, outside the submitted work. M Ajioka reports personal fees from Ono, Novartis, Mitsubishi Tanabe, Pfizer, Daiichi Sankyo, and Otsuka, outside the submitted work. T Anzai reports consulting fees from Terumo, consulting fees from Amgen K.K., personal fees from TOA EIYO, personal fees from Novartis, personal fees from Pharma K.K., personal fees from Bayer, personal fees from Pfizer, personal fees from Bristol-Myers Squibb, personal fees from Ono, personal fees from Otsuka, personal fees from Daiichi Sankyo, personal fees from Mitsubishi Tanabe, personal fees from Boehringer Ingelheim, and personal fees from Takeda, outside the submitted work. T Arikawa reports personal fees from Teijin, outside the submitted work. TH reports personal fees from Otsuka, Ono, AstraZeneca, Medtronic, Daiichi Sankyo, Boehringer Ingelheim, Kowa, Toyobo, Novartis, and TOA EIYO, outside the submitted work. SH reports personal fees from Takeda, Novartis, Otsuka, Bayer, Mitsubishi Tanabe, Daiichi Sankyo, MSD, Teijin, Kowa, Kyowa Kirin, Taisho, Boehringer Ingelheim, Shionogi, Ono, and Sumitomo Dainippon, outside the submitted work. CI reports personal fees from Daiichi Sankyo, Edwards Lifesciences, Bristol-Myers Squibb, Otsuka, Cannon Medical Systems, Sumitomo Dainippon, TOA EIYO, MSD, Pfizer, Boehringer Ingelheim, Teijin, Tsumura, and Novartis, outside the submitted work. K Kimura reports grants from the Research Institute for Production Development, grants from CSL Behring, grants from Mebix, grants from Takeda, grants from Bayer, grants from AstraZeneca, grants from Nippon Shinyaku, grants from Boehringer Ingelheim, grants from Astellas, grants from Abbott Vascular Japan, grants from Medtronic, grants from Kowa, contracts free from National Cerebral and Cardiovascular Center, contracts free from Juntendo, consulting fees from Idorsia Pharmaceuticals Japan, personal fees from Mitsubishi Tanabe, personal fees from Kowa, personal fees from Daiichi Sankyo, personal fees from Bayer, personal fees from AstraZeneca, personal fees from Mochida, personal fees from Astellas, personal fees from MSD, personal fees from Boston Scientific, personal fees from Japan Cardiovascular Research Foundation, personal fees from Sanofi, personal fees from Bristol-Myers Squibb, personal fees from Sumitomo Dainippon, personal fees from Abbott Vascular Japan, personal fees from TOA EIYO, personal fees from Amgen Astellas BioPharma, personal fees from Boehringer Ingelheim, personal fees from Novartis, personal fees from FUJIFILM Toyama Chemical, personal fees from Otsuka, and personal fees from Pfizer, outside the submitted work. K Kinugawa reports personal fees from Otsuka, Nipro, Ono, Abiomed, and AstraZeneca, outside the submitted work. HK reports grants from Japan Society for the Promotion of Science, Japan Agency for Medical Research and Development, Actelion Pharmaceuticals, GSK, and Nakatani foundation, outside the submitted work. TN reports grants from Japan Society for the Promotion of Science, personal fees from Nippon Shinyaku, personal fees from TOA EIYO, and personal fees from Daiichi Sankyo, outside the submitted work. AN reports grants from Grants-in-Aid for Scientific Research, MEXT, Japan, grants from Japan Agency for Medical Research and Development, grants from Japan Heart Foundation, consulting fees from CureApp, personal fees from CureApp, personal fees from Otsuka, personal fees from Kowa, personal fees from Daiichi Sankyo, personal fees from Amgen, support for attending meetings from CureApp, and participation on a Data Safety Monitoring Board or Advisory Board of CureApp, outside the submitted work. S Toyoda reports personal fees from Sumitomo Dainippon, JCR Pharmaceuticals, AstraZeneca, Otsuka, Ono, Sanofi, Daiichi Sankyo, Takeda, Mitsubishi Tanabe, Novartis, Novo Nordisk, Bayer, Pfizer, Bristol-Myers Squibb, and TOA EIYO, outside the submitted work. TU reports personal fees from Ono, Novartis, and Otsuka, outside the submitted work. TW reports personal fees from AstraZeneca, Ono, Novartis, Mitsubishi Tanabe, Takeda, Pfizer, Daiichi Sankyo, Otsuka, and Kowa, outside the submitted work. AY reports personal fees from Ono, Nippon Shinyaku, Novartis, Otsuka, Kowa, Pfizer, Bristol-Myers Squibb, TOA EIYO, AstraZeneca, Amgen, Boehringer Ingelheim, Takeda, Daiichi Sankyo, Bayer, and Mitsubishi Tanabe, outside the submitted work. T Sozu reports grants from Japan Society for the Promotion of Science, reports grants from Japan Agency for Medical Research and Development, consulting fees from Edwards Lifesciences, consulting fees from Ajinomoto Co, consulting fees from Nippon Kayaku, participation on a Data Safety Monitoring Board or Advisory Board of Otsuka, participation on a Data Safety Monitoring Board or Advisory Board of EPS International Holdings, and participation on a Data Safety Monitoring Board or Advisory Board of EPS Associates, outside the submitted work. MK reports grants from the Japanese government, during the conduct of the study; grants from the Japanese government, grants from Japan Heart Foundation, grants from Japan Cardiovascular Research Foundation, grants and personal fees from Takeda, personal fees from Daiichi Sankyo, grants and personal fees from Pfizer, grants and personal fees from Ono, grants and personal fees from AstraZeneca, personal fees from Boehringer Ingelheim, grants from Novartis, grants and personal fees from Mitsubishi Tanabe, personal fees from Kowa, personal fees from Otsuka, grants from Sanofi, personal fees from Amgen, personal fees from Toyama-Kagaku, grants and personal fees from Kureha, outside the submitted work.
Figures


References
-
- Kawaguchi M, Hay I, Fetics B, Kass DA. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: Implications for systolic and diastolic reserve limitations. Circulation. 2003;107:714–720. doi: 10.1161/01.CIR.0000048123.22359.A0. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
