

High level of serum complement 3 is a risk factor for vascular stenosis progression in TA patients receiving tocilizumab: a prospective observational study
- PMID: 37533103
- PMCID: PMC10394800
- DOI: 10.1186/s13075-023-03106-7
High level of serum complement 3 is a risk factor for vascular stenosis progression in TA patients receiving tocilizumab: a prospective observational study
Abstract
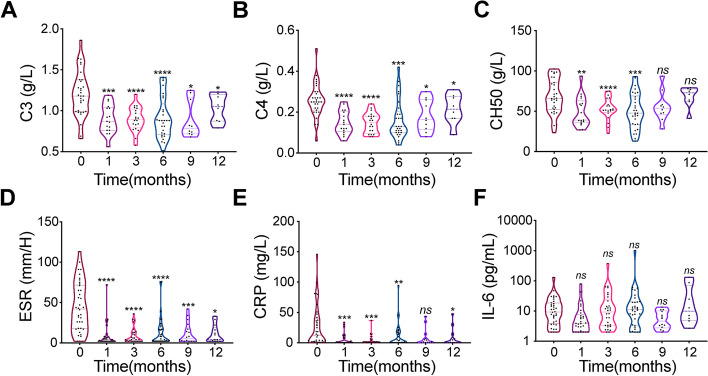
Background: The IL-6R antibody tocilizumab has been proven effective in treating Takayasu arteritis (TA). However, some patients show silent vascular stenosis progression (VSP) despite treatment with tocilizumab. The aim of the study was to explore the related risk factors of VSP in patients treated with tocilizumab.
Methods: Patients receiving tocilizumab were enrolled from the prospective living ongoing East China Takayasu Arteritis cohort. Their medical information was uniformly recorded with a homogenized evaluation method. Magnetic resonant angiography or computed tomographic angiography was employed to monitor VSP during the follow-up period, and Cox regression analysis was performed to explore the related risk factors.
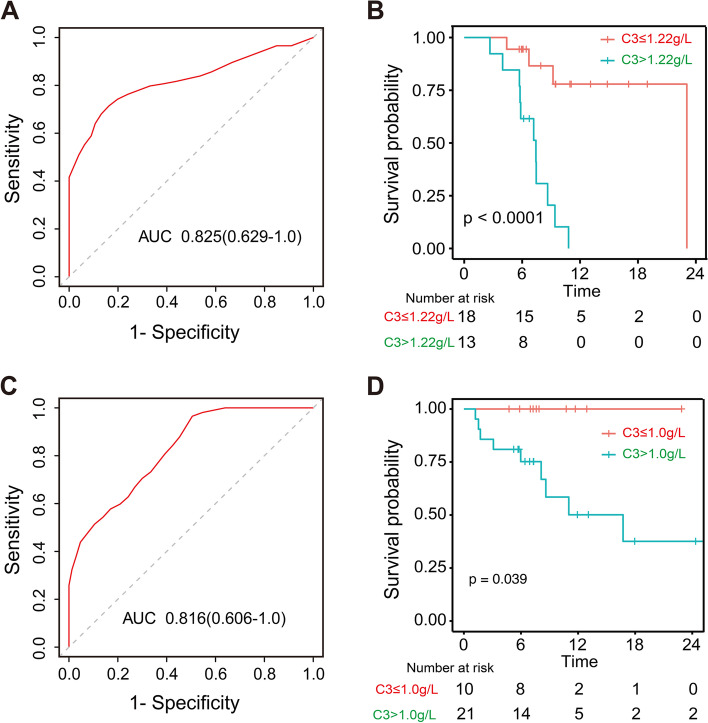
Results: Thirty-eight patients were enrolled, among whom 18 (47.4%) experienced VSP, and seven and three patients experienced new and worsened vascular ischemic symptoms and events (VISE) during follow-up, respectively. The median period for VSP occurrence was 6.9 months during follow-up. Patients with VSP showed higher levels of baseline complement 3 (C3) than those in the patients without VSP. Multivariate Cox regression analysis revealed baseline C3 level (hazard ratio [HR] = 7.05, 95% confidence interval: 1.50-33.07, p = 0.013) was independently associated with VSP, with a cut-off value of 1.22 g/L.
Conclusions: 47.4% of TA patients treated with tocilizumab would suffer VSP. A high C3 level is a risk factor for VSP in TA patients receiving tocilizumab, which may facilitate the option of tocilizumab in the future.
Keywords: Complement 3; Takayasu arteritis; Tocilizumab; Vascular stenosis progression.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
