

Prognosis Analysis of Delayed Call Time for Chest Pain in Patients With Acute ST-Segment Elevation Myocardial Infarction Undergoing Direct Percutaneous Coronary Intervention
- PMID: 37533332
- PMCID: PMC10399249
- DOI: 10.1177/10760296231186811
Prognosis Analysis of Delayed Call Time for Chest Pain in Patients With Acute ST-Segment Elevation Myocardial Infarction Undergoing Direct Percutaneous Coronary Intervention
Abstract
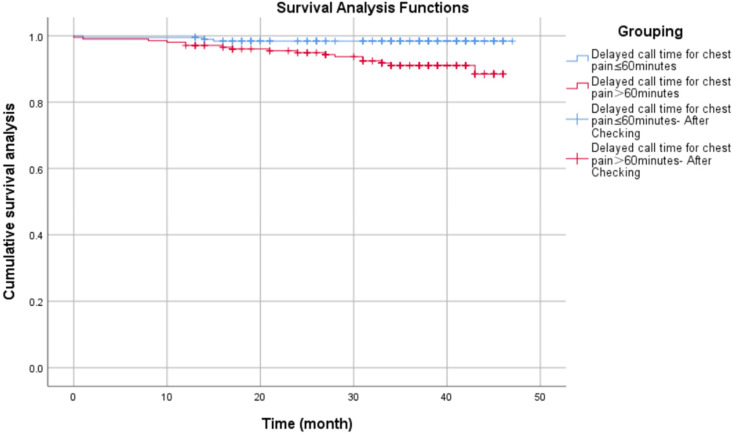
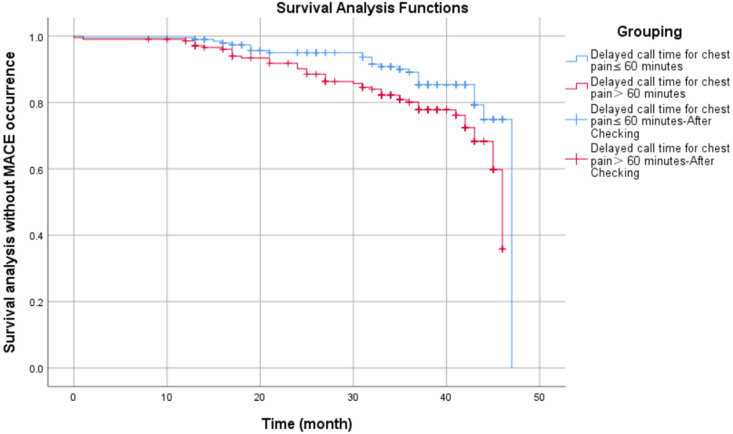
To describe the impact of delayed call time for chest pain in the salvage of ST-segment elevation myocardial infarction (STEMI) patients and its associated independent risk factors, and to identify risk factors associated with cumulative morbidity and mortality in STEMI patients at 4 years after percutaneous coronary intervention (PCI). Retrospective analysis of 398 patients diagnosed with STEMI and treated with emergency PCI within 24 hours of symptom onset in Fuyang People's Hospital from April 2018 to April 2021. The enrolled patients were divided into ≤60 minutes group (193 cases), and > 60 minutes group (205 cases), according to the delayed call time of patients with chest pain. Analysis of basic clinical data, rescue time, and major cardiovascular adverse events in the 2 groups. Multifactorial logistic regression analysis of independent correlates of delayed chest pain calls and Cox proportional risk regression modeling of risk factors for cumulative morbidity and mortality at 4 years after surgery. Compared to the delayed call time ≤ 60 minutes group, the > 60 minutes group had a higher proportion of females, a history of diabetes, rural remote areas, and farmer occupation (P < .05). Binary logistic regression analysis shows the history of diabetes and female as independent risk factors for delayed call time >60 minutes for chest pain. In the delayed call time ≤60 minutes group, the time from symptom onset-to-balloon (S0-to-B) and from symptom onset-to-first medical contact (SO-to-FMC) were smaller than in the delayed call time >60 minutes group (P < .05). The sum of postinfarction angina and major cardiovascular adverse events was lower in the group with delayed call time ≤60 minutes than in the group with delayed call time >60 minutes (P < .05). The Kaplan-Meier survival curve and the survival curve without the occurrence of major adverse cardiovascular events were statistically significant in both groups (P < .05). Multifactorial Cox regression analysis showed that delayed call time for chest pain >60 minutes, left main + 3 branch lesions, and cardiac function Killip ≥ III were all risk factors for cumulative morbidity and mortality at 4 years after PCI in patients with STEMI. Delayed call time for chest pain >60 minutes, left main + 3 branch lesions, and cardiac function Killip ≥ III are all risk factors for cumulative morbidity and mortality in STEMI patients at 4 years after PCI. Reducing the delayed call time for chest pain can improve the long-term prognosis of patients.
Keywords: acute ST-segment elevation myocardial infarction; delayed call time for chest pain; percutaneous coronary intervention; risk factors.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Kristensen SD, Laut KG, Fajadet J, et al. Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011: current status in 37 ESC countries. Eur Heart J. 2014;35(29):1957-1970. - PubMed
-
- Fokkema ML, James SK, Albertsson P, et al. Population trends in percutaneous coronary intervention: 20-year results from the SCAAR (Swedish Coronary Angiography and Angioplasty Registry). J Am Coll Cardiol. 2013;61(12):1222-1230. - PubMed
-
- Vogel B, Claessen BE, Arnold SV, et al. ST-segment elevation myocardial infarction. Nat Rev Dis Primers. 2019;5(1):39. - PubMed
-
- Wei TF, Zhao B, Liu PL, et al. Impact of symptom onset to first medical contact time on the prognosis of patients with acute ST-segment elevation myocardial infarction. Zhonghua Xin Xue Guan Bing Za Zhi. 2017;45(5):393-398. - PubMed
-
- Hochberg CP, Jacobs AK. Prehospital delay in patients with ST-segment elevation myocardial infarction: time for change. Coron Artery Dis. 2018;29(5):368-370. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
