

Top Ten Pearls for a Successful Transtibial Pull-Out Repair of Medial Meniscal Posterior Root Tears With a Concomitant Centralization Stitch
- PMID: 37533905
- PMCID: PMC10390883
- DOI: 10.1016/j.eats.2023.02.053
Top Ten Pearls for a Successful Transtibial Pull-Out Repair of Medial Meniscal Posterior Root Tears With a Concomitant Centralization Stitch
Abstract
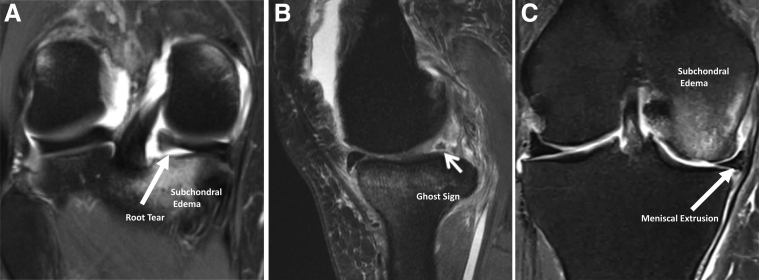
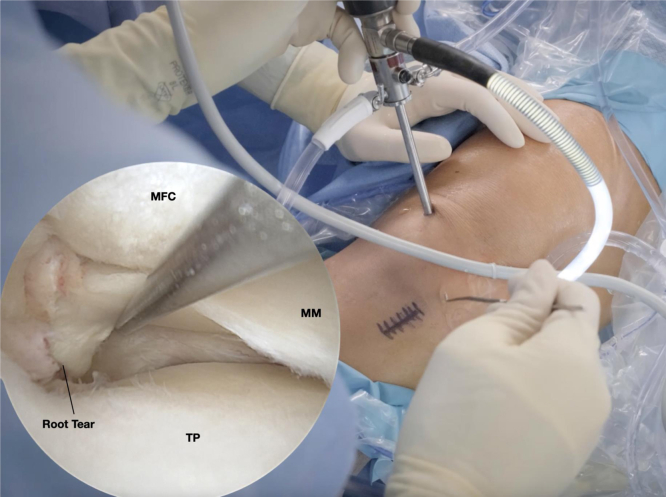
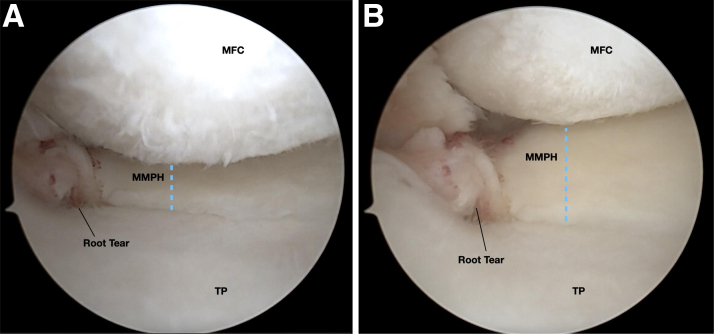
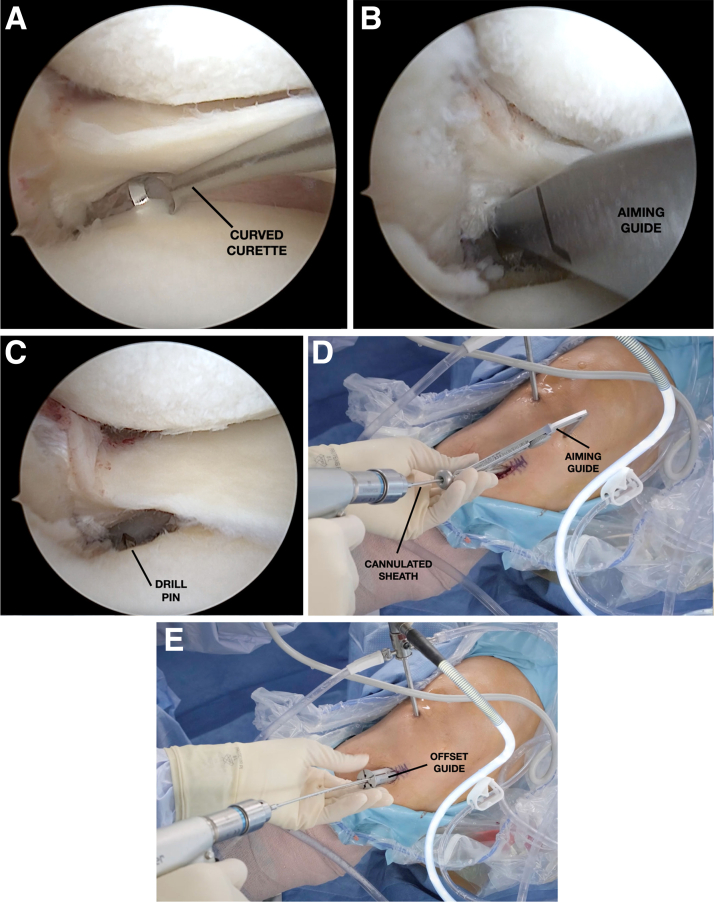
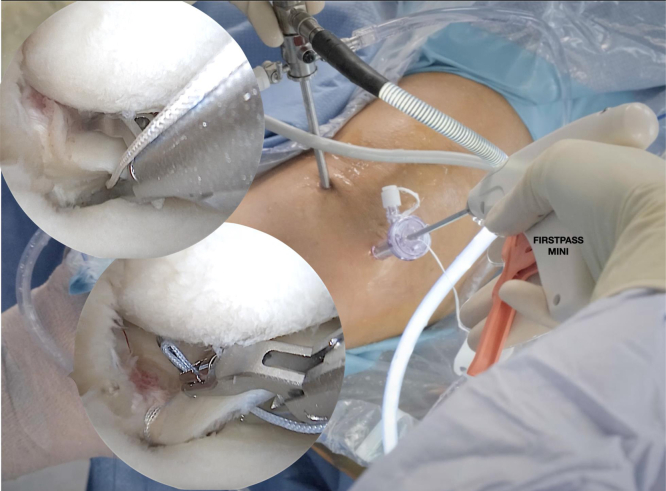
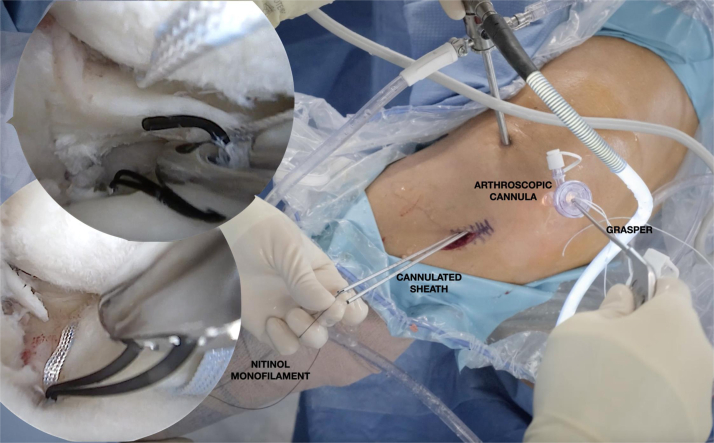
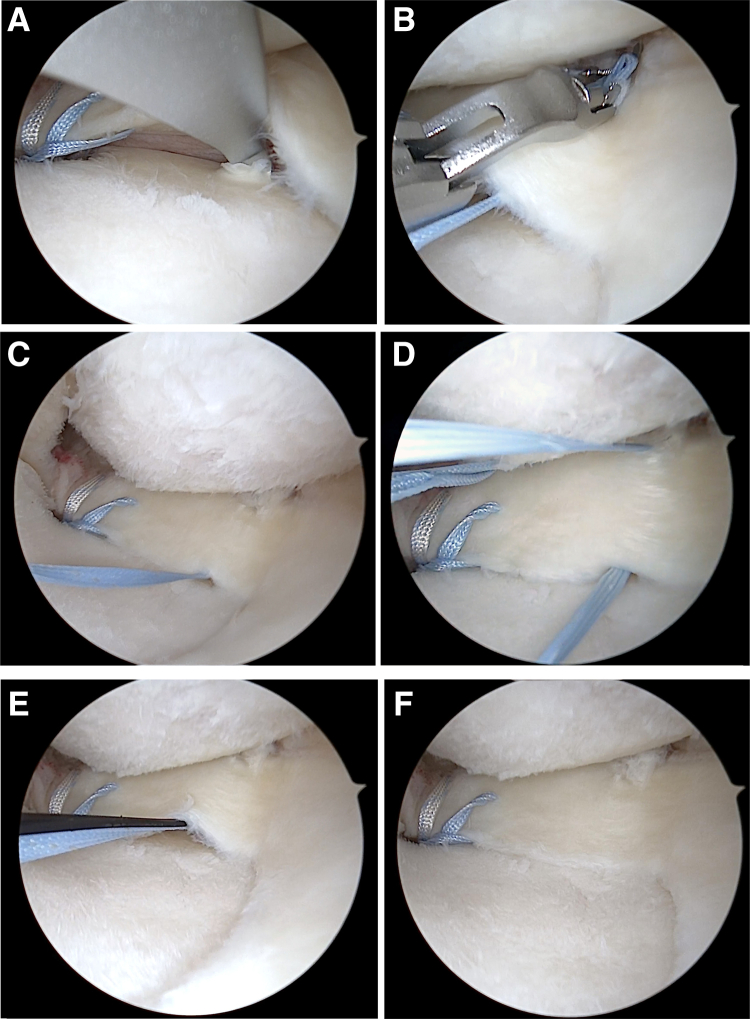
Although historically overlooked, medial meniscus posterior root (MMPR) tears are now increasingly recognized as a substantial cause of biomechanical impairment and morbidity. MMPR tears, when left untreated, are strongly correlated to meniscal extrusion and ultimately lead to altered kinematics and loading functionally equivalent to a total meniscectomy. To prevent progressive joint degeneration and alleviate pain while re-establishing native joint kinematics, MMPR repair is generally recommended in appropriately selected patients. In this Technical Note, the authors describe a detailed checklist with 10 crucial points of emphasis when performing the gold-standard transtibial pull-out repair of the MMPR, with an additional centralization stitch, providing technical pearls backed up by previous literature and ample experience treating this condition.
© 2023 The Authors.
Figures

Similar articles
-
Utilization of Transtibial Centralization Suture Best Minimizes Extrusion and Restores Tibiofemoral Contact Mechanics for Anatomic Medial Meniscal Root Repairs in a Cadaveric Model.Am J Sports Med. 2019 Jun;47(7):1591-1600. doi: 10.1177/0363546519844250. Epub 2019 May 15. Am J Sports Med. 2019. PMID: 31091129
-
Different Suture Materials for Arthroscopic Transtibial Pull-out Repair of Medial Meniscal Posterior Root Tears: A Human Biomechanical Study.Orthop J Sports Med. 2019 Sep 30;7(9):2325967119873274. doi: 10.1177/2325967119873274. eCollection 2019 Sep. Orthop J Sports Med. 2019. PMID: 31632997 Free PMC article.
-
Examining the Efficacy of Medial Meniscus Posterior Root Repair: A Meta-analysis and Systematic Review of Biomechanical and Clinical Outcomes.Am J Sports Med. 2023 Jun;51(7):1914-1926. doi: 10.1177/03635465221077271. Epub 2022 Apr 6. Am J Sports Med. 2023. PMID: 35384728
-
Biomechanical evaluation of a transtibial pull-out meniscal root repair: challenging the bungee effect.Am J Sports Med. 2014 Dec;42(12):2988-95. doi: 10.1177/0363546514549447. Epub 2014 Sep 19. Am J Sports Med. 2014. PMID: 25239930
-
Current Reviews in Musculoskeletal Medicine: Current Controversies for Treatment of Meniscus Root Tears.Curr Rev Musculoskelet Med. 2022 Aug;15(4):231-243. doi: 10.1007/s12178-022-09759-2. Epub 2022 Apr 27. Curr Rev Musculoskelet Med. 2022. PMID: 35476312 Free PMC article. Review.
Cited by
-
Placing the transtibial centralisation stitch at the posterior horn of the medial meniscus best restores tibiofemoral contact mechanics and extrusion following medial meniscus posterior root tears: An in vitro biomechanical study using porcine knee joints.J Exp Orthop. 2025 Mar 22;12(1):e70217. doi: 10.1002/jeo2.70217. eCollection 2025 Jan. J Exp Orthop. 2025. PMID: 40123681 Free PMC article.
-
Minimally Invasive Unicompartmental Articular Resurfacing.Arthrosc Tech. 2024 Dec 10;14(4):103351. doi: 10.1016/j.eats.2024.103351. eCollection 2025 Apr. Arthrosc Tech. 2024. PMID: 40453032 Free PMC article.
-
Review of the Development of Meniscus Centralization.Curr Rev Musculoskelet Med. 2024 Aug;17(8):303-312. doi: 10.1007/s12178-024-09905-y. Epub 2024 May 17. Curr Rev Musculoskelet Med. 2024. PMID: 38760631 Free PMC article. Review.
-
[Refixation of a posterior medial root lesion in combination with centralization by a meniscotibial suture].Oper Orthop Traumatol. 2025 Jun;37(3-4):254-265. doi: 10.1007/s00064-024-00858-6. Epub 2024 Aug 22. Oper Orthop Traumatol. 2025. PMID: 39172276 German.
-
Diagnosis and Treatment Strategies of Meniscus Root Tears: A Scoping Review.Orthop J Sports Med. 2024 Nov 1;12(11):23259671241283962. doi: 10.1177/23259671241283962. eCollection 2024 Nov. Orthop J Sports Med. 2024. PMID: 39493310 Free PMC article.
References
-
- Bhatia S., LaPrade C.M., Ellman M.B., LaPrade R.F. Meniscal root tears: Significance, diagnosis, and treatment. Am J Sports Med. 2014;42:3016–3030. - PubMed
-
- Cinque M.E., Chahla J., Moatshe G., Faucett S.C., Krych A.J., LaPrade R.F. Meniscal root tears: a silent epidemic. Br J Sports Med. 2018;52:872–876. - PubMed
-
- Allaire R., Muriuki M., Gilbertson L., Harner C.D. Biomechanical consequences of a tear of the posterior root of the medial meniscus. Similar to total meniscectomy. J Bone Joint Surg Am. 2008;90:1922–1931. - PubMed
LinkOut - more resources
Full Text Sources
