

Modified Arthroscopic Latissimus Dorsi Transfer at the Infraspinatus Footprint With Anterior Extracortical Fixation
- PMID: 37533920
- PMCID: PMC10391566
- DOI: 10.1016/j.eats.2023.03.014
Modified Arthroscopic Latissimus Dorsi Transfer at the Infraspinatus Footprint With Anterior Extracortical Fixation
Abstract
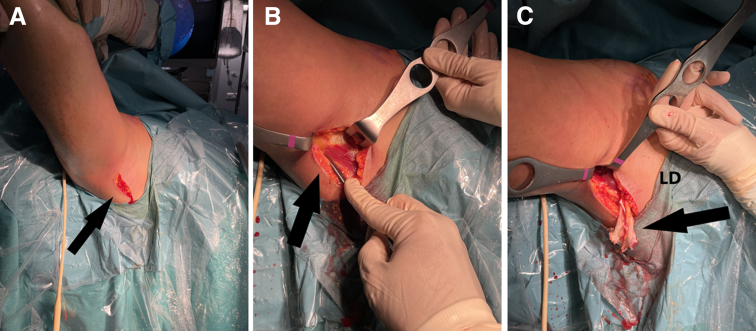
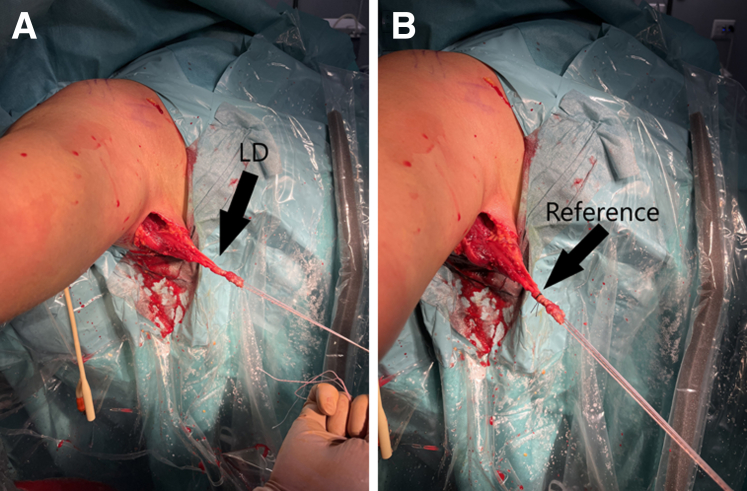
Massive irreparable cuff tears may represent as many as 20% to 40% of total cases of operated rotator cuff tears and can be a challenging clinical problem. Many treatment options have been proposed for their treatment. Among these options, latissimus dorsi tendon transfer can be considered a good alternative, especially in young patients before they develop glenohumeral arthritic changes. This technique aims at rebalancing the shoulder with a functioning subscapularis muscle and restoring both active external rotation and elevation with the aid of a properly functioning deltoid muscle. The modified arthroscopic latissimus dorsi transfer at the infraspinatus footprint with anterior extracortical fixation rebalances the pair of forces acting on the shoulder, stabilizing it in the transverse plane, minimizing the risk of latissimus dorsi transferred rupture and associated complications.
© 2023 The Authors.
Figures









References
-
- Kany J., Grimberg J., Amaravathi R.S., Sekaran P., Scorpie D., Werthel J.D. Arthroscopically-assisted latissimus dorsi transfer for irreparable rotator cuff insufficiency: Modes of failure and clinical correlation. Arthroscopy. 2018;34:1139–1150. - PubMed
-
- Lädermann A., Denard P.J., Collin P. Massive rotator cuff tears: Definition and treatment. Int Orthop. 2015;39:2403–2414. - PubMed
-
- Parsons I.M., Apreleva M., Fu F.H., Woo S.L. The effect of rotator cuff tears on reaction forces at the glenohumeral joint. J Orthop Res. 2002;20:439–446. - PubMed
-
- Mulieri P., Dunning P., Klein S., Pupello D., Frankle M. Reverse shoulder arthroplasty for the treatment of irreparable rotator cuff tear without glenohumeral arthritis. J Bone Joint Surg Am. 2010;92:2544–2556. - PubMed
LinkOut - more resources
Full Text Sources
