

AML consolidation therapy: timing matters
- PMID: 37535164
- PMCID: PMC10590325
- DOI: 10.1007/s00432-023-05115-0
AML consolidation therapy: timing matters
Abstract
Purpose: Infections due to severe neutropenia are the most common therapy-associated causes of mortality in patients with acute myeloid leukemia (AML). New strategies to lessen the severity and duration of neutropenia are needed.
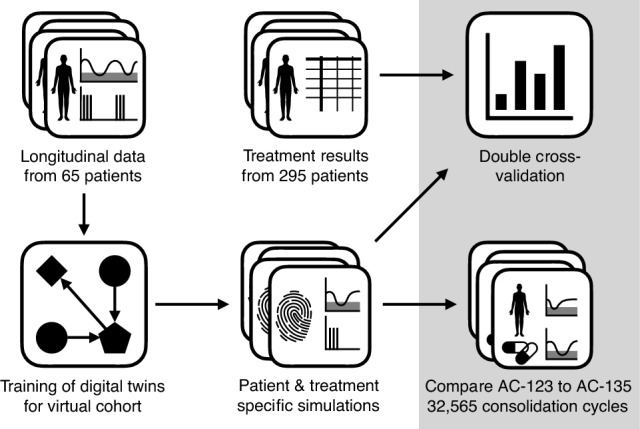
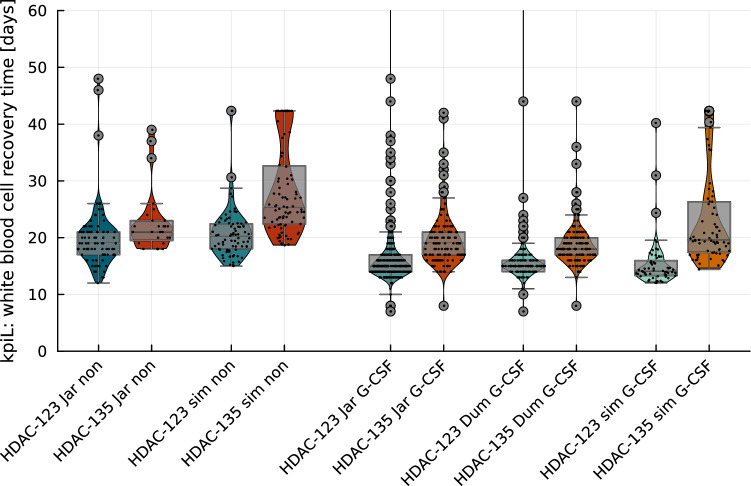
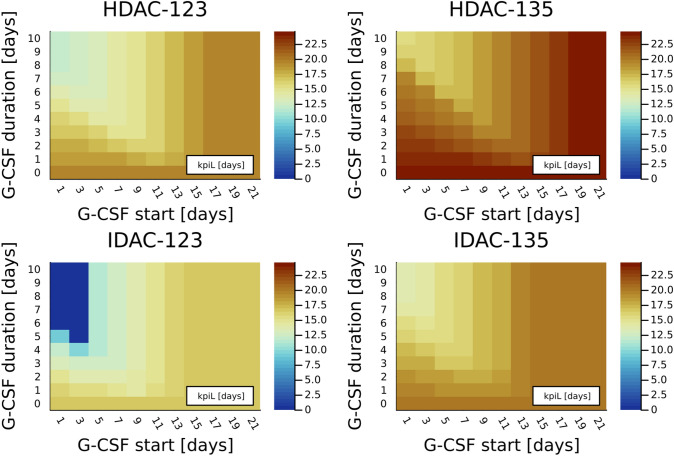
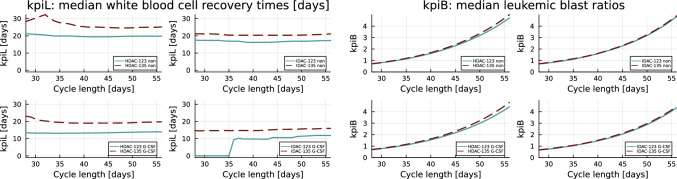
Methods: Cytarabine is commonly used for AML consolidation therapy; we compared high- and intermediate-dose cytarabine administration on days 1, 2, and 3 (AC-123) versus days 1, 3, and 5 (AC-135) in consolidation therapy of AML. Recently, clinical trials demonstrated that high-dose AC-123 resulted in a shortened white blood cell (WBC) recovery time compared with high-dose AC-135. Our main hypothesis is that this is also the case for different cytarabine dosage, granulocyte colony-stimulating factor (G-CSF) administration, and cycle lengths. We analyzed 334 treatment schedules on virtual cohorts of digital twins.
Results: Comparison of 32,565 simulated consolidation cycles resulted in a reduction in the WBC recovery time for AC-123 in 99.6% of the considered cycles (median reduction 3.5 days) without an increase in the number of leukemic blasts (lower value in 94.2% of all cycles), compared to AC-135.
Conclusion: Our numerical study supports the use of AC-123 plus G-CSF as standard conventional AML consolidation therapy to reduce the risk for life-threatening infectious complications.
Keywords: Acute myeloid leukemia; Chemotherapy; Digital twin; Mathematical modeling; Myelosuppression; Neutropenia.
© 2023. The Author(s).
Conflict of interest statement
DM consults for Abbvie, Beigene, BMS, Gilead, Janssen, Novartis, and Takeda. HD consults Abbvie, Agios, Amgen, Astellas, AstraZeneca, Berlin-Chemie, Bristol Myers Squibb, Celgene, Daiichi Sankyo, GEMoaB, Gilead, Janssen, Jazz Pharmaceuticals, Novartis, Servier, Stemline, and Syndax. His institute has been receiving support from Abbvie, Agios, Amgen, Astellas, Bristol Myers Squibb, Jazz Pharmaceuticals, Kronos-Bio, Novartis, and Pfizer. CR is on the advisory boards of Abbvie, Astellas, BMS, Jazz Pharma, Novartis, Servier, and Takeda; his institution is supported by Abbvie, Astellas, BMS, Jazz Pharmaceuticals, and Iqvia. PYD consults for Daiichi-Sankyo, Jazz Pharmaceutical, Astellas, Abbvie, BMS, Janssen, and Novartis; his institution is supported by Astellas, Roche, Gilead, Daiichi-Sankyo, BMS, Servier, and Novartis. All other authors declare no competing interests.
Figures

References
-
- Burnett AK, Russell NH, Hills RK, Hunter AE, Kjeldsen L, Yin J, Gibson BES, Wheatley K, Milligan D (2013) Optimization of chemotherapy for younger patients with acute myeloid leukemia: results of the Medical Research Council AML15 trial. J Clin Oncol 31(27):3360–3368. 10.1200/JCO.2012.47.4874 - DOI - PubMed
-
- Chulián S, Martínez-Rubio Á, Rosa M, Pérez-García VM (2022) Mathematical models of leukaemia and its treatment: a review. SeMA J 79(3):441–486. 10.1007/s40324-022-00296-z - DOI
-
- Clairambault J (2009) Modelling physiological and pharmacological control on cell proliferation to optimise cancer treatments. Math Model Nat Phenom 4(3):12–67. 10.1051/mmnp/20094302 - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
