

Development of a Prediction Score for Evaluation of Extubation Readiness in Neurosurgical Patients with Mechanical Ventilation
- PMID: 37535470
- PMCID: PMC10566588
- DOI: 10.1097/ALN.0000000000004721
Development of a Prediction Score for Evaluation of Extubation Readiness in Neurosurgical Patients with Mechanical Ventilation
Abstract
Background: There is no widely accepted consensus on the weaning and extubating protocols for neurosurgical patients, leading to heterogeneity in clinical practices and high rates of delayed extubation and extubation failure-related health complications.
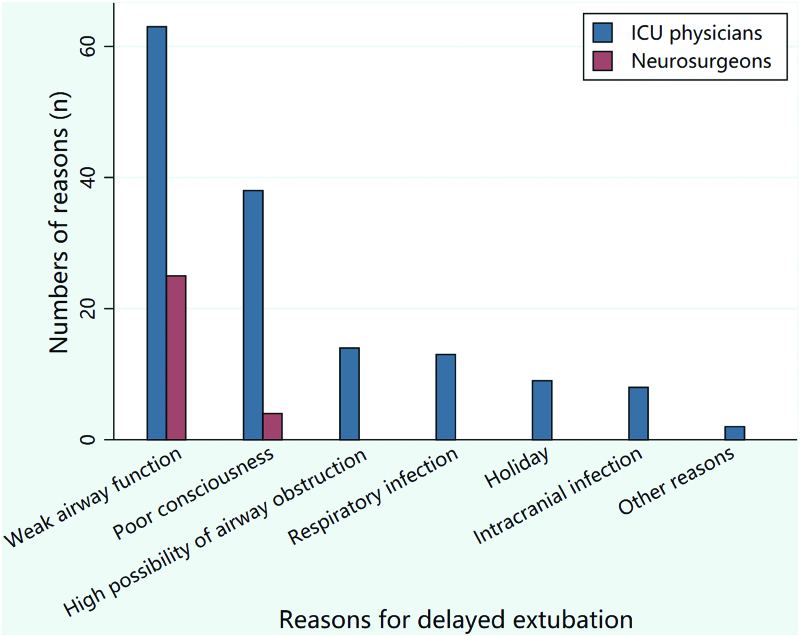
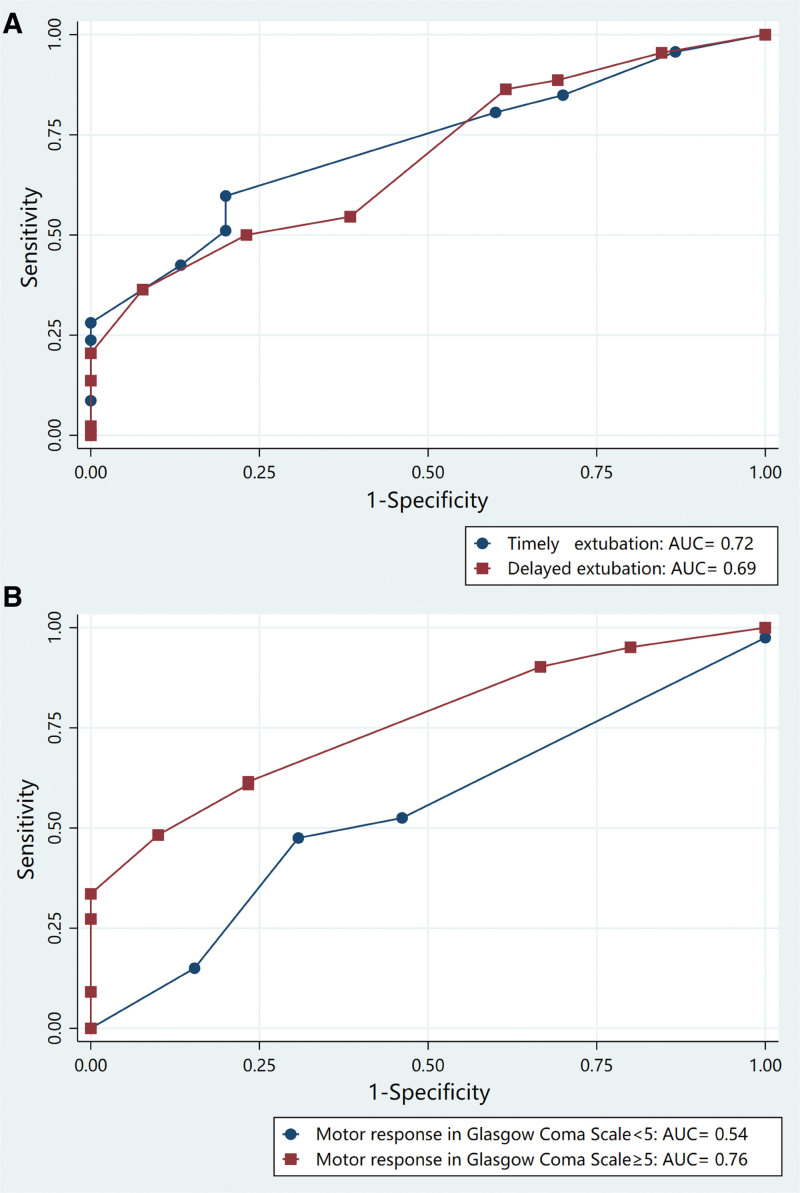
Methods: In this single-center prospective observational diagnostic study, mechanically ventilated neurosurgical patients with extubation attempts were consecutively enrolled for 1 yr. Responsive physicians were surveyed for the reasons for delayed extubation and developed the Swallowing, Tongue protrusion, Airway protection reflected by spontaneous and suctioning cough, and Glasgow Coma Scale Evaluation (STAGE) score to predict the extubation success for neurosurgical patients already meeting other general extubation criteria.
Results: A total of 3,171 patients were screened consecutively, and 226 patients were enrolled in this study. The rates of delayed extubation and extubation failure were 25% (57 of 226) and 19% (43 of 226), respectively. The most common reasons for the extubation delay were weak airway-protecting function and poor consciousness. The area under the receiver operating characteristics curve of the total STAGE score associated with extubation success was 0.72 (95% CI, 0.64 to 0.79). Guided by the highest Youden index, the cutoff point for the STAGE score was set at 6 with 59% (95% CI, 51 to 66%) sensitivity, 74% (95% CI, 59 to 86%) specificity, 90% (95% CI, 84 to 95%) positive predictive value, and 30% (95% CI, 21 to 39%) negative predictive value. At STAGE scores of 9 or higher, the model exhibited a 100% (95% CI, 90 to 100%) specificity and 100% (95% CI, 72 to 100%) positive predictive value for predicting extubation success.
Conclusions: After a survey of the reasons for delayed extubation, the STAGE scoring system was developed to better predict the extubation success rate. This scoring system has promising potential in predicting extubation readiness and may help clinicians avoid delayed extubation and failed extubation-related health complications in neurosurgical patients.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc., on behalf of the American Society of Anesthesiologists.
Conflict of interest statement
The authors declare no competing interests.
Figures





Similar articles
-
Predicting Extubation Outcome by Cough Peak Flow Measured Using a Built-in Ventilator Flow Meter.Respir Care. 2017 Dec;62(12):1505-1519. doi: 10.4187/respcare.05460. Epub 2017 Sep 12. Respir Care. 2017. PMID: 28900041
-
Clinical Scoring and Ultrasound-Based Diaphragm Assessment in Predicting Extubation Failure in Neurointensive Care Unit: A Single-Center Observational Study.Neurocrit Care. 2023 Dec;39(3):690-696. doi: 10.1007/s12028-023-01695-4. Epub 2023 Mar 1. Neurocrit Care. 2023. PMID: 36859489
-
Extubation Failure in Brain-injured Patients: Risk Factors and Development of a Prediction Score in a Preliminary Prospective Cohort Study.Anesthesiology. 2017 Jan;126(1):104-114. doi: 10.1097/ALN.0000000000001379. Anesthesiology. 2017. PMID: 27749290
-
Who Is Safe to Extubate in the Neuroscience Intensive Care Unit?Semin Respir Crit Care Med. 2017 Dec;38(6):830-839. doi: 10.1055/s-0037-1608773. Epub 2017 Dec 20. Semin Respir Crit Care Med. 2017. PMID: 29262440 Review.
-
Predictive factors of weaning from mechanical ventilation and extubation outcome: A systematic review.J Crit Care. 2018 Dec;48:56-62. doi: 10.1016/j.jcrc.2018.08.023. Epub 2018 Aug 20. J Crit Care. 2018. PMID: 30172034
Cited by
-
Analyzing Risk Factors for Delayed Extubation Following Posterior Approach Surgery for Congenital Scoliosis: A Retrospective Cohort Study.Global Spine J. 2025 May;15(4):2051-2061. doi: 10.1177/21925682241282275. Epub 2024 Sep 2. Global Spine J. 2025. PMID: 39223805 Free PMC article.
-
Using ML techniques to predict extubation outcomes for patients with central nervous system injuries in the Yun-Gui Plateau.Sci Rep. 2025 May 22;15(1):17773. doi: 10.1038/s41598-025-98861-9. Sci Rep. 2025. PMID: 40404881 Free PMC article.
-
Extubation Failure and Timing to Tracheostomy in Children Surviving Acute Neurological Injury.Children (Basel). 2025 Apr 30;12(5):586. doi: 10.3390/children12050586. Children (Basel). 2025. PMID: 40426765 Free PMC article.
-
Current advances in neurocritical care.J Intensive Med. 2024 Jul 3;5(1):23-31. doi: 10.1016/j.jointm.2024.04.005. eCollection 2025 Jan. J Intensive Med. 2024. PMID: 39872833 Free PMC article. Review.
-
Predictive value of cough peak flow for successful extubation in mechanically ventilated patients after craniotomy: a single-centre prospective diagnostic study.BMJ Open. 2025 Jan 2;15(1):e088219. doi: 10.1136/bmjopen-2024-088219. BMJ Open. 2025. PMID: 39753249 Free PMC article.
References
-
- Pelosi P, Ferguson ND, Frutos-Vivar F, Anzueto A, Putensen C, Raymondos K, Apezteguia C, Desmery P, Hurtado J, Abroug F, Elizalde J, Tomicic V, Cakar N, Gonzalez M, Arabi Y, Moreno R, Esteban A; Ventila Study Group: Management and outcome of mechanically ventilated neurologic patients. Crit Care Med 2011; 39:1482–92 - PubMed
-
- Karanjia N, Nordquist D, Stevens R, Nyquist P: A clinical description of extubation failure in patients with primary brain injury. Neurocrit Care 2011; 15:4–12 - PubMed
-
- Ko R, Ramos L, Chalela JA: Conventional weaning parameters do not predict extubation failure in neurocritical care patients. Neurocrit Care 2009; 10:269–73 - PubMed
-
- MacIntyre N: Discontinuing mechanical ventilatory support. Chest 2007; 132:1049–56 - PubMed
-
- Thille AW, Harrois A, Schortgen F, Brun-Buisson C, Brochard L: Outcomes of extubation failure in medical intensive care unit patients. Crit Care Med 2011; 39:2612–8 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
