

Risks of Uterine Perforation and Expulsion Associated With Intrauterine Devices
- PMID: 37535968
- PMCID: PMC10424817
- DOI: 10.1097/AOG.0000000000005299
Risks of Uterine Perforation and Expulsion Associated With Intrauterine Devices
Abstract
Objective: The APEX-IUD (Association of Perforation and Expulsion of Intrauterine Devices) study evaluated the association of postpartum timing of intrauterine device (IUD) insertion, breastfeeding, heavy menstrual bleeding, and IUD type (levonorgestrel-releasing vs copper) with risks of uterine perforation and IUD expulsion in usual clinical practice. We summarize the clinically important findings to inform counseling and shared decision making.
Methods: APEX-IUD was a real-world (using U.S. health care data) retrospective cohort study of individuals aged 50 years and younger with IUD insertions between 2001 and 2018 and with electronic health record data. Cumulative incidences of uterine perforation and IUD expulsion were calculated. Adjusted hazard ratios (aHRs) and 95% CIs were estimated from proportional hazards models with control of confounding.
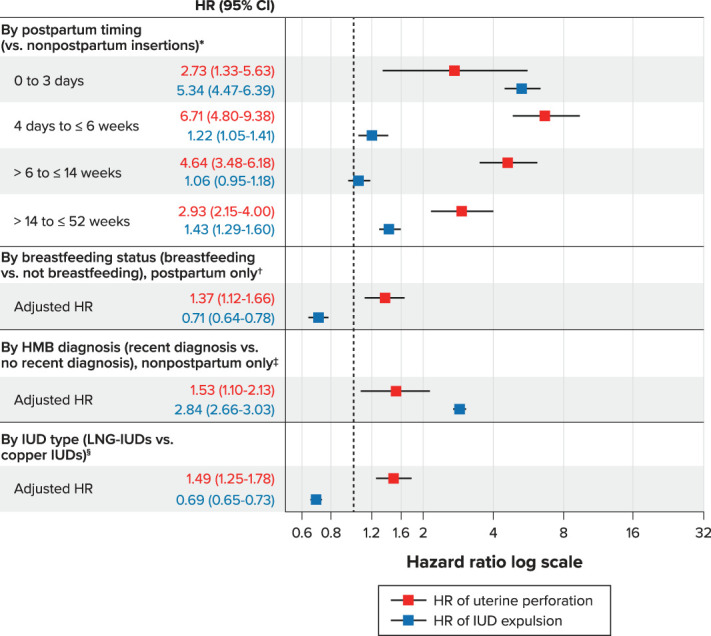
Results: Among the study population of 326,658, absolute risk of uterine perforation was low overall (cumulative incidence, 0.21% [95% CI 0.19-0.23%] at 1 year and 0.61% [95% CI 0.56-0.66% at 5 years]) but was elevated for IUDs inserted during time intervals within 1 year postpartum, particularly among those between 4 days and 6 weeks postpartum (aHR 6.71, 95% CI 4.80-9.38), relative to nonpostpartum insertions. Among postpartum insertions, IUD expulsion risk was greatest for insertions in the immediate postpartum period (0-3 days after delivery) compared with nonpostpartum (aHR 5.34, 95% CI 4.47-6.39). Postpartum individuals who were breastfeeding had a slightly elevated risk of perforation and lowered risk of expulsion than those not breastfeeding. Among nonpostpartum individuals, those with a heavy menstrual bleeding diagnosis were at greater risk of expulsion than those without (aHR 2.84, 95% CI 2.66-3.03); heavy menstrual bleeding also was associated with a slightly elevated perforation risk. There was a slightly elevated perforation risk and slightly lower expulsion risk associated with levonorgestrel-releasing IUDs compared with copper IUDs.
Conclusion: Absolute risk of adverse outcomes with IUD insertion is low. Clinicians should be aware of the differences in risks of uterine perforation and expulsion associated with IUD insertion during specific postpartum time periods and with a heavy menstrual bleeding diagnosis. This information should be incorporated into counseling and decision making for patients considering IUD insertion.
Funding source: Bayer AG.
Clinical trial registration: EU PAS register, EUPAS33461.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Financial Disclosure Susan Reed has received funding from the National Institutes of Health (NIH) and Bayer, as well as royalties from UpToDate on chapters related to endometrial hyperplasia. Jeffrey F. Peipert receives research support from Bayer, Merck, and CooperSurgical, and has served on advisory boards for Bayer, CooperSurgical, and OCON. Darios Getahun receives research support from NIH, NIEH, DHHS, NICHD, Patient-Centered Outcomes Research Institute, Garfield Memorial Fund, Bayer AG, and HOLOGIC, Inc. Jennifer Gatz disclosed money was paid to her institution from Cook, Lily, and Janssen. Michael J. Fassett receives research support from Garfield Memorial Fund, Bayer AG, and HOLOGIC, Inc. Federica Pisa, Juliane Schoendorf, and Yesmean Wahdan are employees of Bayer, the marketing authorization holder for 3 IUD brands, among others, that were included in this study. Jinyi Wang and Mary S. Anthony are employed at RTI Health Solutions, and Mary E. Ritchey was employed at RTI Health Solutions at the time the analysis was conducted. This organization worked under contract with Bayer to conduct the analyses. No payment or support of any kind was received for drafting or review of this manuscript. Tina Raine-Bennett, an employee of KPNC during the conduct of the study, is currently an employee of Medicines360, a marketing authorization holder for one of the IUD brands included in this study. The other authors did not report any potential conflicts of interest.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
