

Early Diagnosis of Tuberous Sclerosis Complex: Prenatal Diagnosis
- PMID: 37536734
- PMCID: PMC10494953
- DOI: 10.3174/ajnr.A7952
Early Diagnosis of Tuberous Sclerosis Complex: Prenatal Diagnosis
Erratum in
-
Erratum.AJNR Am J Neuroradiol. 2025 Apr 2;46(4):859. doi: 10.3174/ajnr.A8711. AJNR Am J Neuroradiol. 2025. PMID: 40097187 Free PMC article. No abstract available.
Abstract
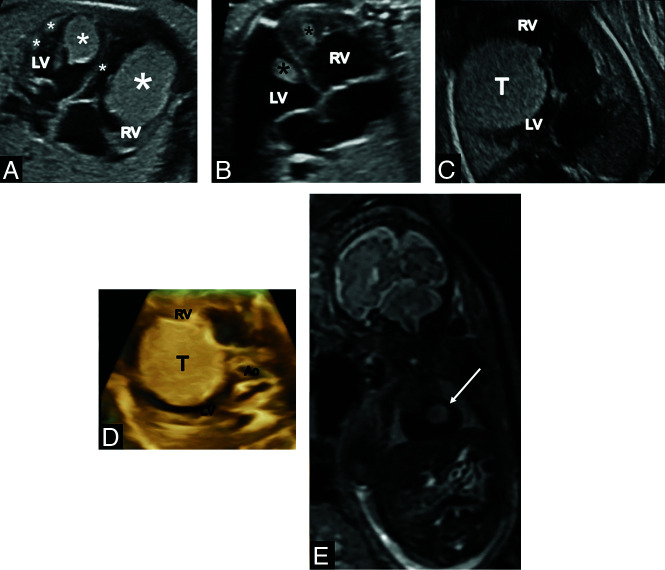
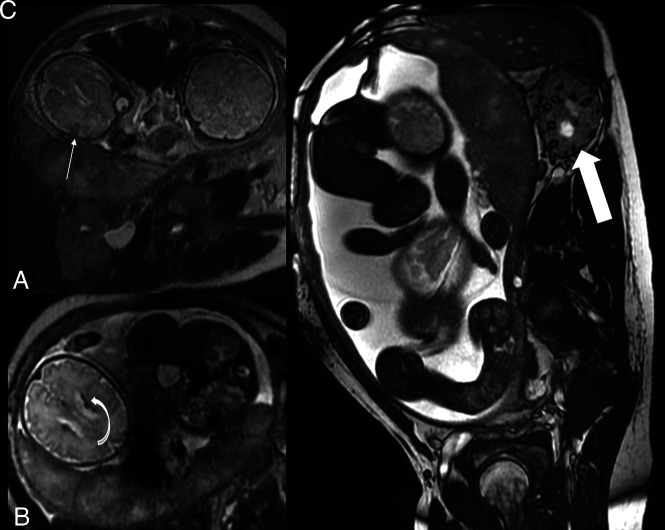
Background and purpose: Strong emphasis has been placed recently on early (4 postnatal months) detection of tuberous sclerosis complex and the introduction of antiepileptic treatment before seizure onset. This objective can be achieved prenatally: Cardiac rhabdomyomas and the major diagnostic tuberous sclerosis complex sign are detected during fetal ultrasound, and prenatal MR imaging allows detection of cerebral major manifestations: cortical tubers, subependymal nodules, and subependymal giant cell astrocytomas.
Materials and methods: We retrospectively reviewed 50 fetuses with ultrasound-detected cardiac tumors at 19-36 gestational weeks (median, 31 weeks). MR imaging with the use of 1.5T scanners was performed at 24-37 gestational weeks (median, 34 weeks).
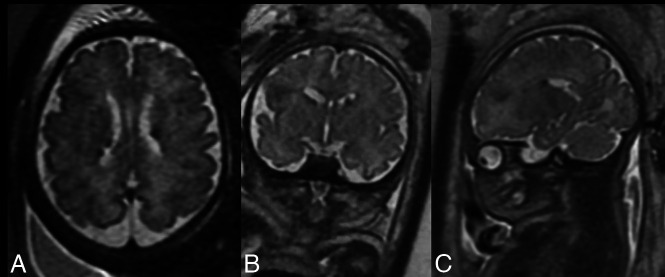
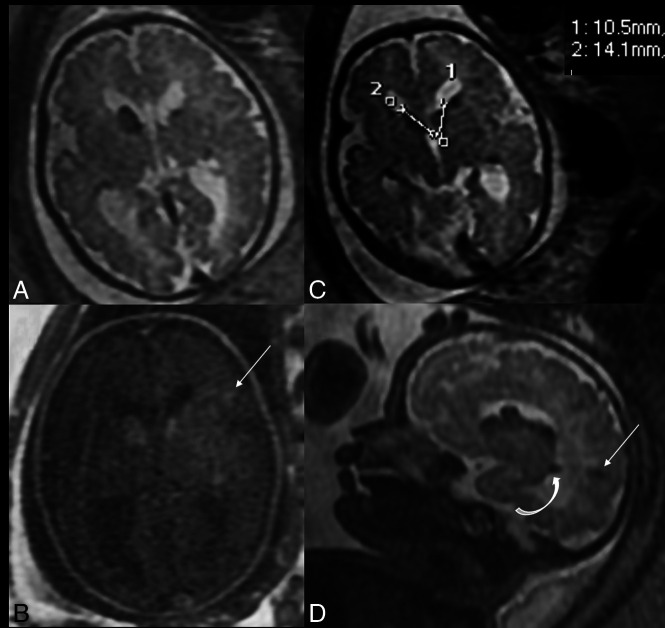
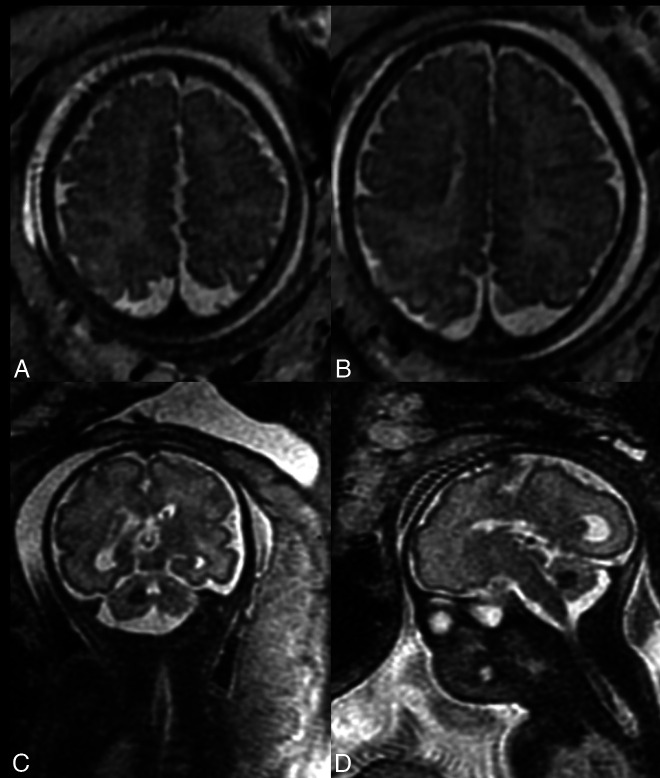
Results: In 11 fetuses (22%), cardiac tumors remained the only criterion. In remaining 39 fetuses (78%), MR imaging revealed a prenatal diagnosis of tuberous sclerosis complex, having shown an additional 1-3 major criteria: subependymal nodules in all cases (39/39 = 100.0%), subependymal giant cell astrocytomas in 6 (6/39 = 15.4%), and cortical tubers in 24 (24/39 = 61.5%). Radial migration lines and cerebellar tuber, not published so far, were shown in 1 case each.
Conclusions: A schedule of proper care of children with tuberous sclerosis complex can be established during the perinatal period due to education of women to report for mandatory ultrasound examinations during pregnancy, the good quality of ultrasound, and referral to MR imaging if a cardiac tumor is depicted on ultrasound. Gynecologists and pediatric cardiologists performing fetal ultrasound and radiologists performing prenatal MR imaging are a key to early diagnosis of tuberous sclerosis complex in many cases.
© 2023 by American Journal of Neuroradiology.
Figures
References
-
- Hinton RB, Prakash A, Romp RL, et al. ; International Tuberous Sclerosis Consensus Group. Cardiovascular manifestations of tuberous sclerosis complex and summary of the revised diagnostic criteria and surveillance and management recommendations from the International Tuberous Sclerosis Consensus Group. J Am Heart Assoc 2014;3:e001493 10.1161/JAHA.114.001493 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical