

Successful surgical treatment of postmyomectomy uterine diverticulum: a case report
- PMID: 37537601
- PMCID: PMC10398967
- DOI: 10.1186/s12905-023-02539-1
Successful surgical treatment of postmyomectomy uterine diverticulum: a case report
Abstract
Background: Uterine diverticulum is classified into congenital and acquired types. The acquired type is caused by caesarean scar syndrome, which occurs after caesarean section. There are no detailed reports on diverticulum after enucleation of uterine fibroids. Most cases are treated with hysteroscopy or laparoscopy, but a management consensus is lacking. We treated a patient with a uterine diverticulum that had formed after uterine fibroid enucleation by combining hysteroscopic and laparoscopic treatments.
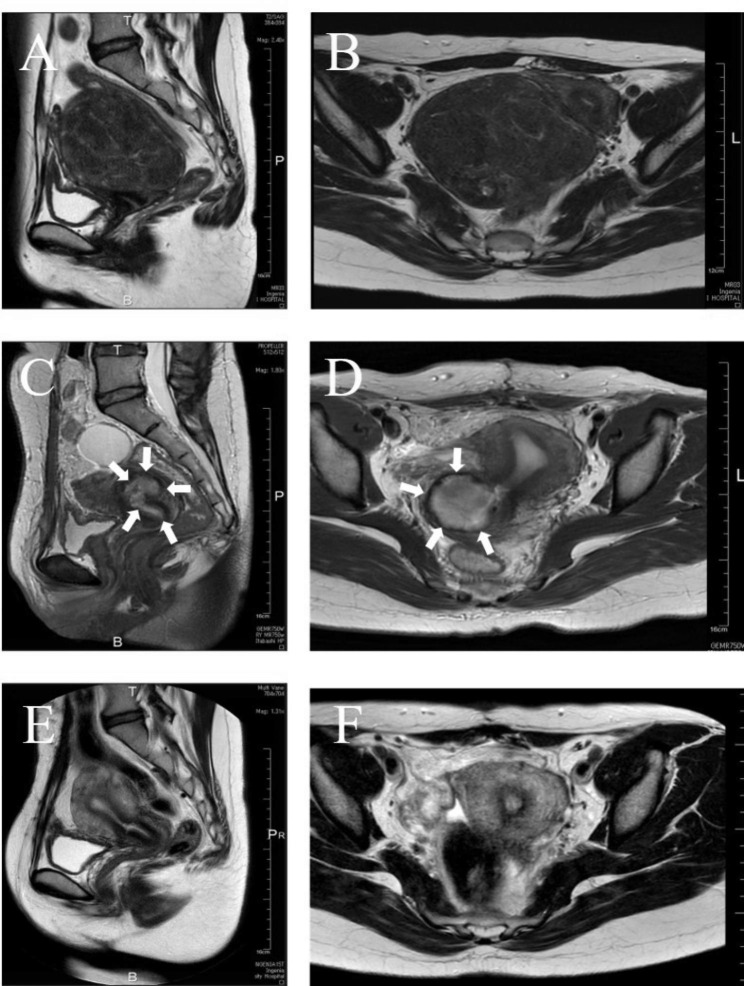
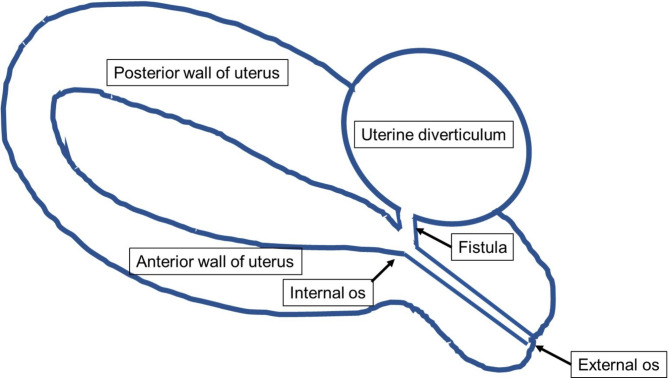
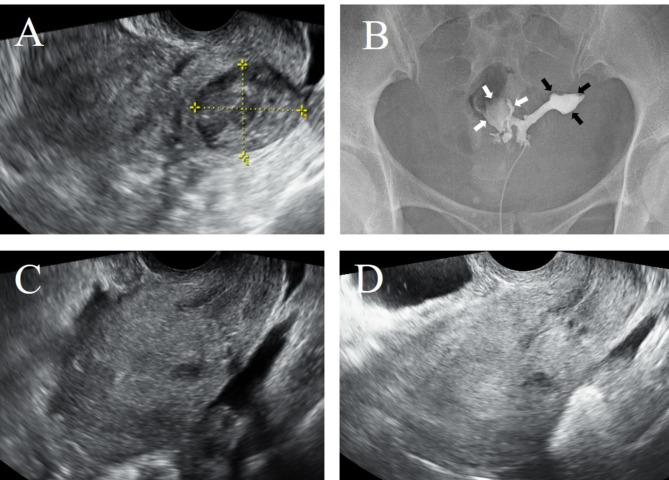
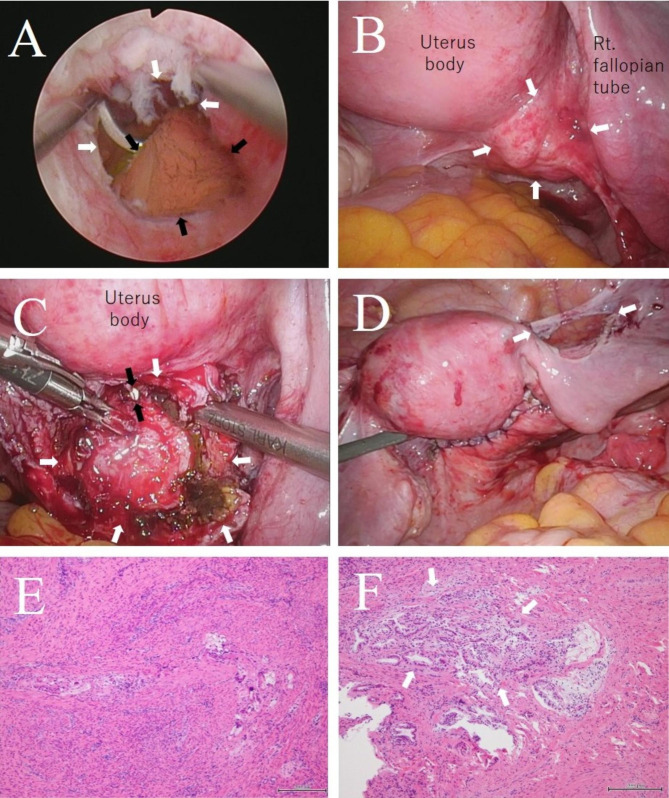
Case presentation: The patient was a 37-year-old Japanese woman, G1P0. A previous doctor had performed abdominal uterine myomectomy for a pedunculated subserosal uterine fibroid on the right side of the posterior wall of the uterus near the internal cervical os. Menstruation resumed postoperatively, but a small amount of dark-red bleeding persisted. MRI two months after the myomectomy revealed a diverticulum-like structure 3 cm in diameter, communicating with the uterine lumen, on the right side of the posterior wall of the uterus. Under suspicion of uterine diverticulum after uterine fibroid enucleation, the patient sought treatment at our hospital approximately four months after the myomectomy. Through a flexible hysteroscope, a 5-mm-diameter fistula was observed in the posterior wall of the uterus, and a contrast-enhanced pocket, measuring approximately 3 cm, was located behind it. Uterine diverticulum following enucleation of a uterine fibroid was diagnosed, and surgery was thus deemed necessary. The portion entering the fistula on the internal cervical os side was resected employing a hysteroscope. Intra-abdominal findings included a 4-cm mass lesion on the posterior wall on the right side of the uterus. The mass was opened, and the cyst capsule was removed. A 5-mm fistula was detected and closed with sutures. Resuturing was not performed after dissection of the right round ligament due to tension. The postoperative course has been good to date, with no recurrence.
Conclusion: Uterine diverticula after myomectomy may be treated with a combined laparoscopic and hysteroscopic approach, similar to caesarean scar syndrome.
Keywords: Hysteroscopy; Laparoscopy; Postmyomectomy; Surgical treatment; Uterine diverticulum.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors have no competing interests to disclose.
Figures
References
-
- Tanimura S, Funamoto H, Hosono T, Shitano Y, Nakashima M, Ametani Y, Nakano T. New diagnostic criteria and operative strategy for cesarean scar syndrome: endoscopic repair for secondary infertility caused by cesarean scar defect. J Obstet Gynaecol Res. 2015;41:1363–69. doi: 10.1111/jog.12738. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
