

Microvascular function and inflammatory activation in Takotsubo cardiomyopathy
- PMID: 37537779
- PMCID: PMC10567652
- DOI: 10.1002/ehf2.14461
Microvascular function and inflammatory activation in Takotsubo cardiomyopathy
Abstract
Aims: The aim of this study was to determine microvascular function in the acute phase of Takotsubo syndrome (TTS) and to identify inflammatory mediators that could reflect TTS-induced pathology.
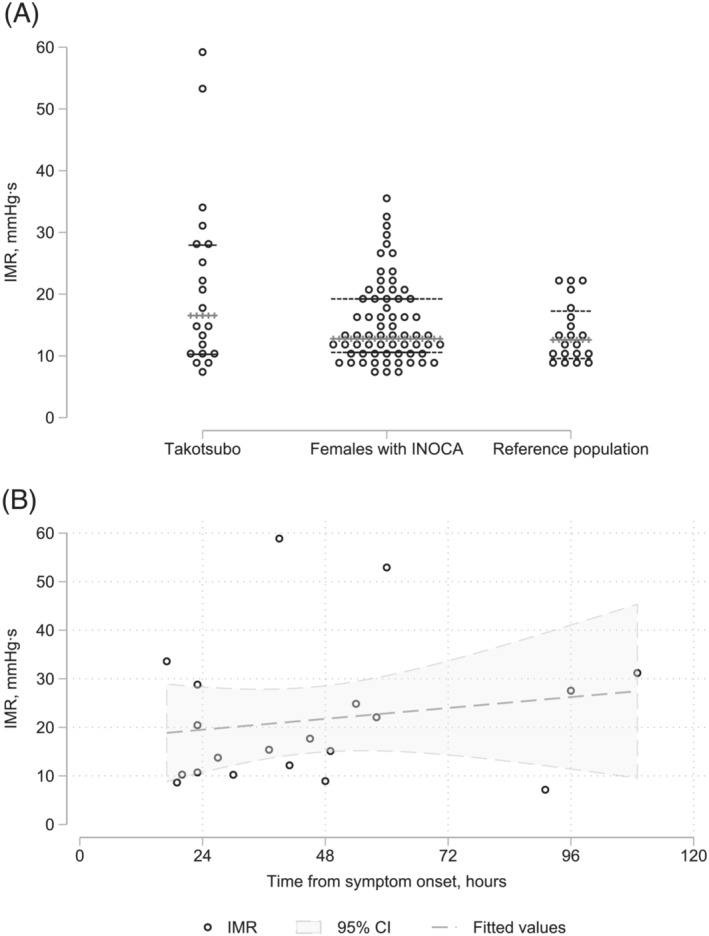
Methods and results: The study included 20 females [median age 65 years; interquarile range (IQR) = 58-70 years] with TTS according to the Mayo diagnostic criteria. During heart catheterization, we determined the index of microvascular resistance (IMR) and drew blood samples almost simultaneously from the aorta and coronary sinus. Cardiac magnetic resonance imaging (MRI) was done in the acute phase. We present descriptive coronary physiology and cardiac MRI data and compare inflammatory biomarkers between samples from the aorta, coronary sinus, and venous samples after 3 months using the Wilcoxon signed-rank test. For comparison, we also analysed the actual biomarkers in venous blood from 15 healthy female controls. A supplementary analysis explored Spearman's rank correlation between the inflammatory biomarkers, IMR, MRI data, and cardiac biomarkers. The median IMR was 16.5 mmHg·s (IQR = 10.5-28.2 mmHg·s), which was only slightly higher than that in the reference populations. Seven (35%) of the study subjects had IMR > 25 mmHg·s, suggesting a microvascular dysfunction. IMR was not affected by time from symptom onset. According to MRI, the apical region of the left ventricle was affected in 65% of the subjects. The median ejection fraction was 41% (IQR = 31-48%). Biomarker analyses revealed elevation of markers for extracellular matrix remodelling and fibrosis, inflammation, immune activation, and upstream inflammation as compared with healthy controls. Only the levels of interleukin (IL)-1 receptor antagonist and soluble T-cell immunoglobulin mucin domain-3 (sTIM-3) were higher in the coronary sinus than in the aorta. No variable was significantly correlated with IMR. The IL-6 level in the aorta was inversely correlated with the left ventricular ejection fraction. Growth differentiation factor-15, osteoprotegerin, and von Willebrand factor levels in both aorta and coronary sinus were positively correlated with N-terminal-pro-brain-natriuretic peptide, while the correlations of IL-6 and sTIM-3 with N-terminal-pro-brain-natriuretic peptide were restricted to the aorta and coronary sinus, respectively. While most of the markers were within normal limits after 3 months, matrix metalloproteinase-9 increased during follow-up to reach levels higher than those in the healthy controls.
Conclusion: The median IMR was only slightly elevated in this study, but about one-third of the patients had values indicating microvascular dysfunction. The present study supports the involvement of several inflammatory pathways in TTS, including monocyte/macrophage activation, with sTIM-3 as a potential novel marker.
Keywords: Index of microvascular resistance (IMR); Inflammatory markers; Takotsubo cardiomyopathy.
© 2023 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Uribarri A, Núñez‐ Gil IJ, Conty DA, Vedia O, Almendro‐ Delia M, Durán Cambra A, Martin‐ Garcia AC, Barrionuevo‐ Sánchez M, Martínez‐ Sellés M, Raposeiras‐Roubín S. Short‐ and long‐ term prognosis of patients with Takotsubo syndrome based on different triggers: importance of the physical nature. JAMA. 2019; 8: e013701. - PMC - PubMed
-
- Ghadri JR, Kato K, Cammann VL, Gili S, Jurisic S, Di Vece D, Candreva A, Ding KJ, Micek J, Szawan KA. Long‐term prognosis of patients with Takotsubo syndrome. J Am Coll Cardiol. 2018; 72: 874–882. - PubMed
-
- Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, Cammann VL, Sarcon A, Geyer V, Neumann CA. Clinical features and outcomes of Takotsubo (stress) cardiomyopathy. N Engl J Med. 2015; 373: 929–938. - PubMed
-
- Sharkey SW, Windenburg DC, Lesser JR, Maron MS, Hauser RG, Lesser JN, Haas TS, Hodges JS, Maron BJ. Natural history and expansive clinical profile of stress (Takotsubo) cardiomyopathy. J Am Coll Cardiol. 2010; 55: 333–341. - PubMed
LinkOut - more resources
Full Text Sources
