

Development of artificial intelligence tools for invasive Doppler-based coronary microvascular assessment
- PMID: 37538145
- PMCID: PMC10393887
- DOI: 10.1093/ehjdh/ztad030
Development of artificial intelligence tools for invasive Doppler-based coronary microvascular assessment
Abstract
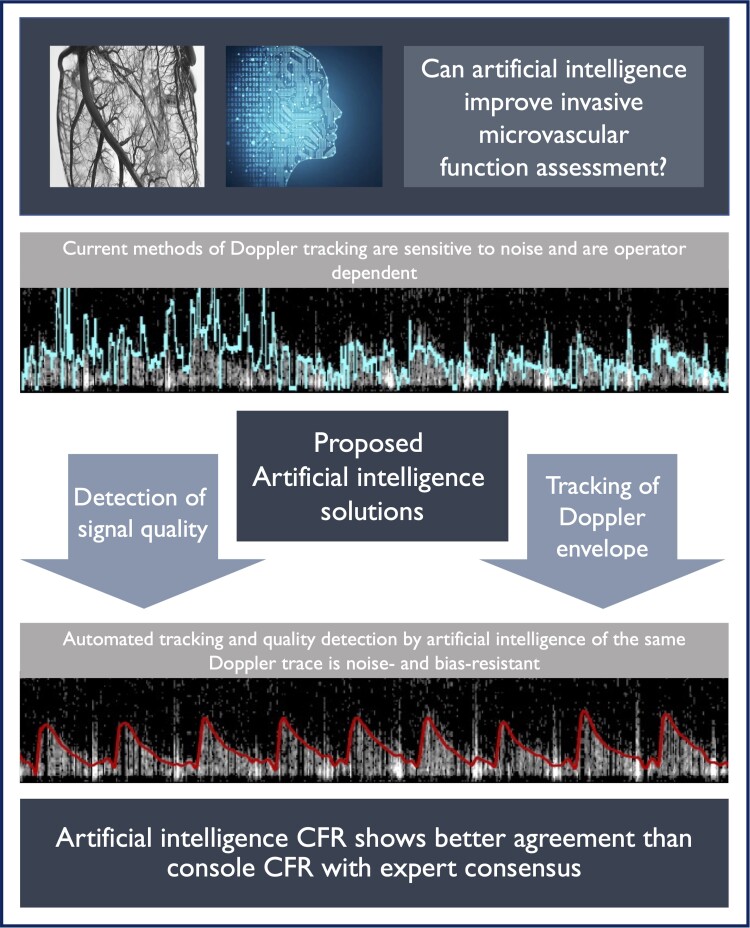
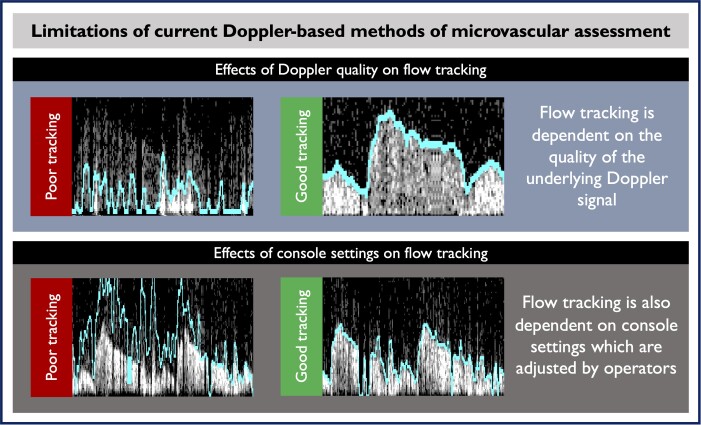
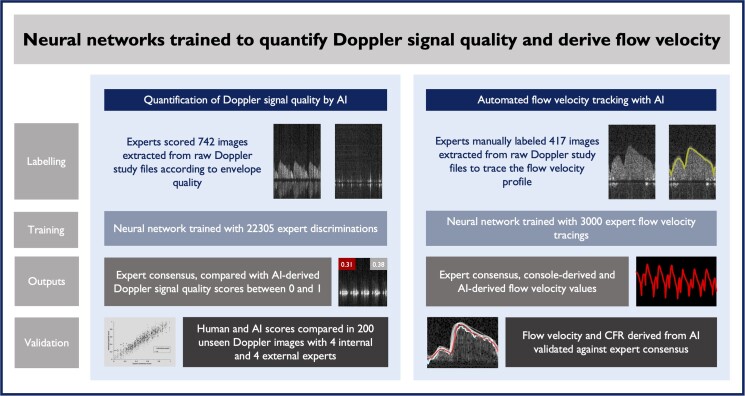
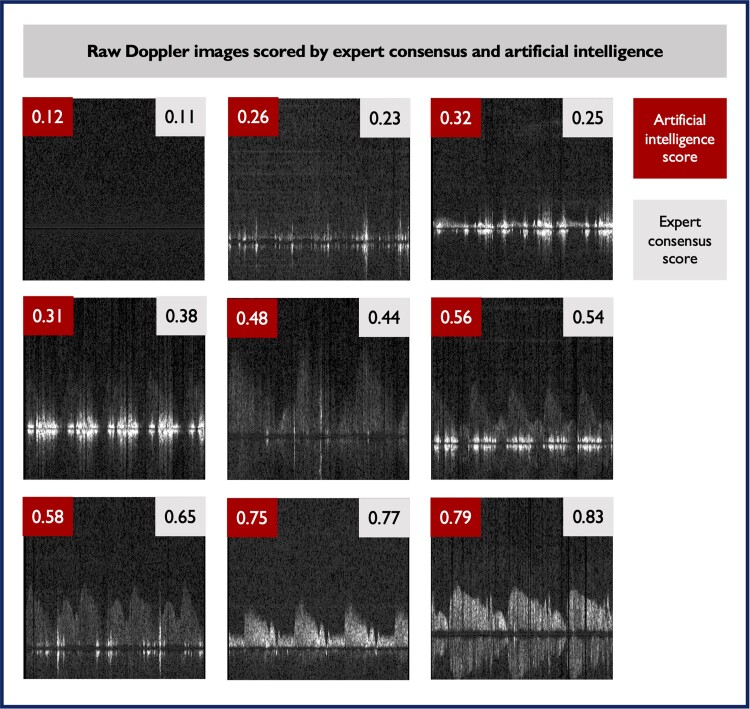
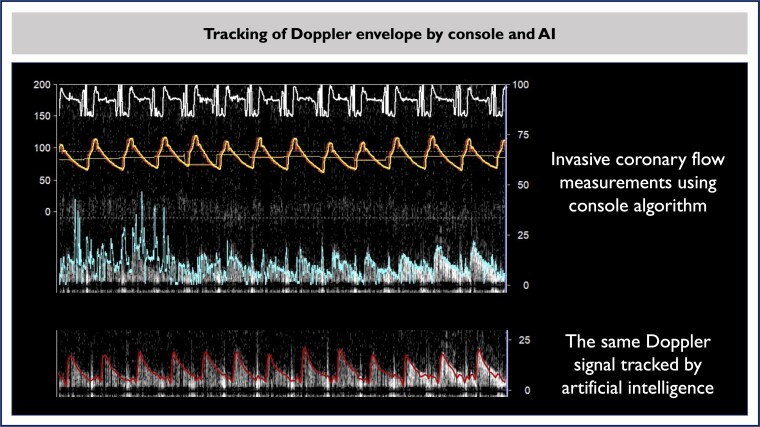
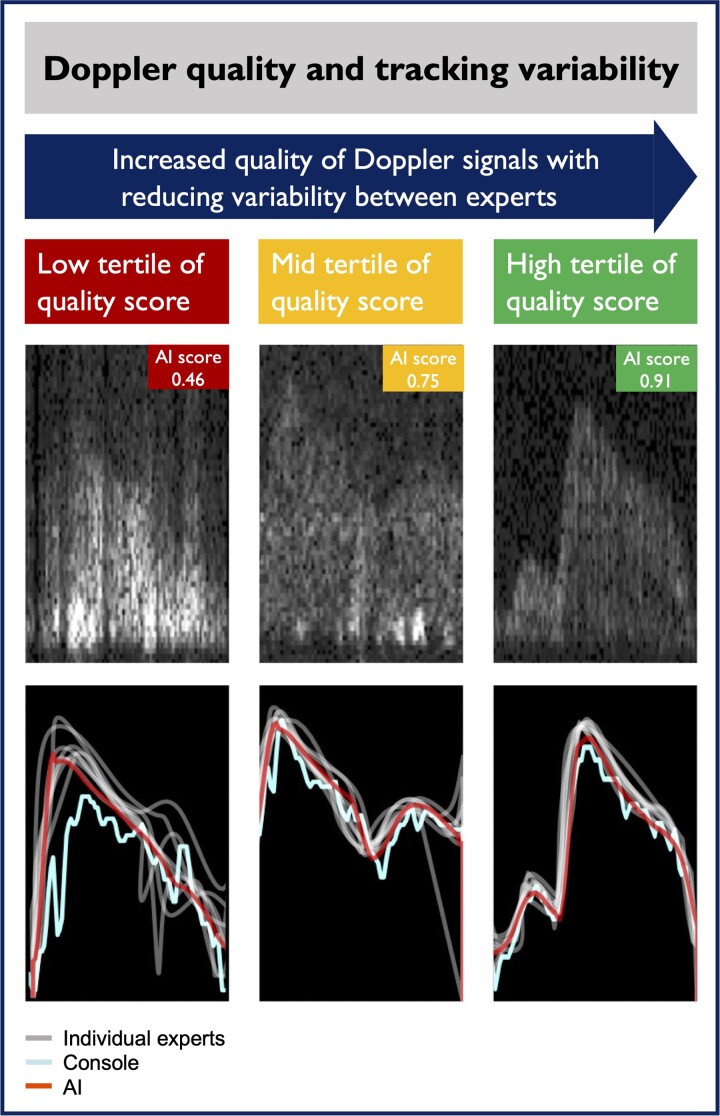
Aims: Coronary flow reserve (CFR) assessment has proven clinical utility, but Doppler-based methods are sensitive to noise and operator bias, limiting their clinical applicability. The objective of the study is to expand the adoption of invasive Doppler CFR, through the development of artificial intelligence (AI) algorithms to automatically quantify coronary Doppler quality and track flow velocity.
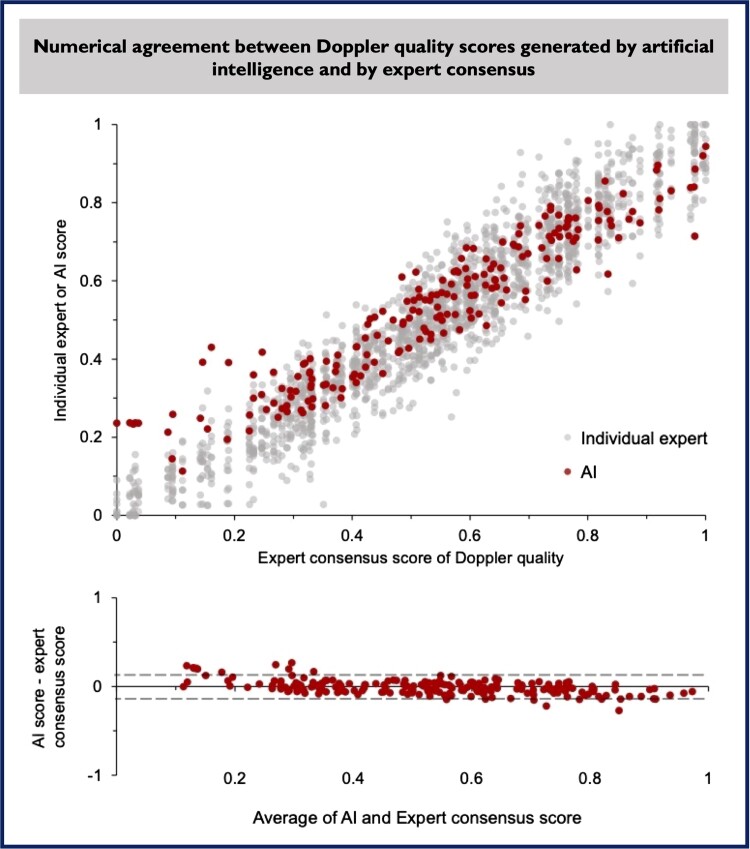
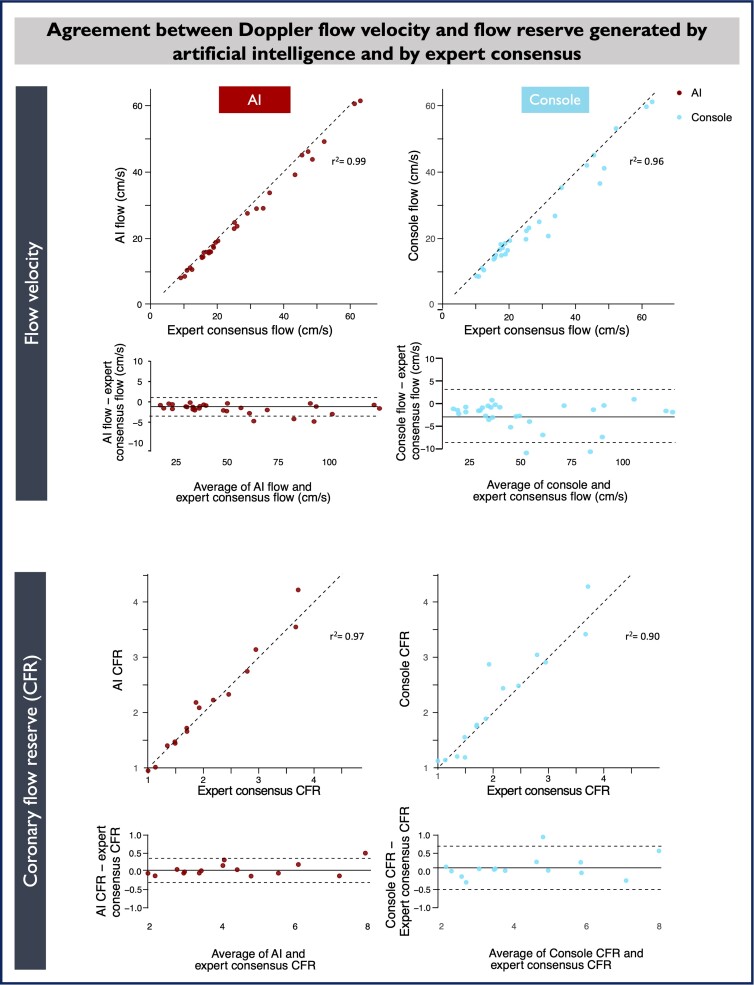
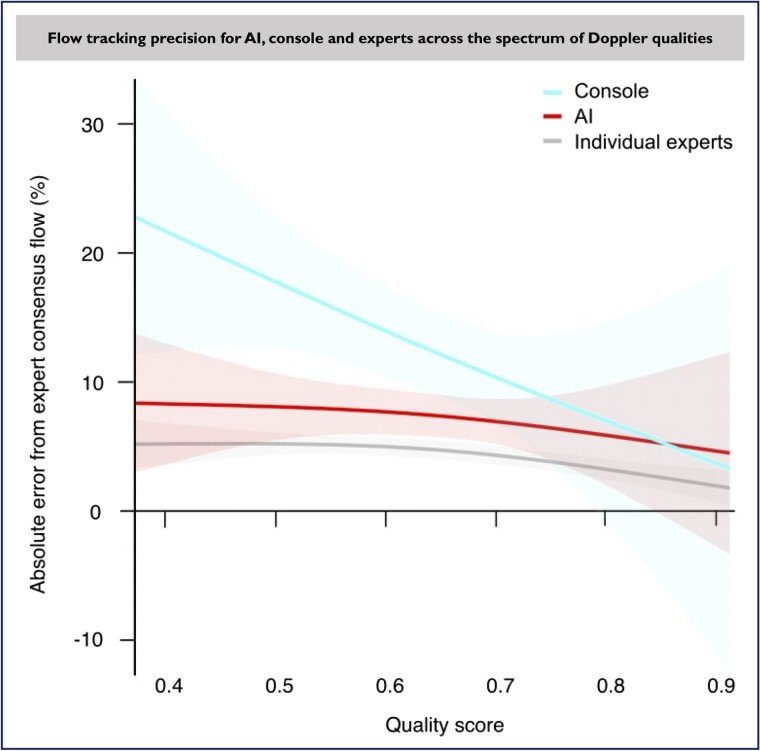
Methods and results: A neural network was trained on images extracted from coronary Doppler flow recordings to score signal quality and derive values for coronary flow velocity and CFR. The outputs were independently validated against expert consensus. Artificial intelligence successfully quantified Doppler signal quality, with high agreement with expert consensus (Spearman's rho: 0.94), and within individual experts. Artificial intelligence automatically tracked flow velocity with superior numerical agreement against experts, when compared with the current console algorithm [AI flow vs. expert flow bias -1.68 cm/s, 95% confidence interval (CI) -2.13 to -1.23 cm/s, P < 0.001 with limits of agreement (LOA) -4.03 to 0.68 cm/s; console flow vs. expert flow bias -2.63 cm/s, 95% CI -3.74 to -1.52, P < 0.001, 95% LOA -8.45 to -3.19 cm/s]. Artificial intelligence yielded more precise CFR values [median absolute difference (MAD) against expert CFR: 4.0% for AI and 7.4% for console]. Artificial intelligence tracked lower-quality Doppler signals with lower variability (MAD against expert CFR 8.3% for AI and 16.7% for console).
Conclusion: An AI-based system, trained by experts and independently validated, could assign a quality score to Doppler traces and derive coronary flow velocity and CFR. By making Doppler CFR more automated, precise, and operator-independent, AI could expand the clinical applicability of coronary microvascular assessment.
Keywords: Angina; Artificial intelligence; Coronary; Diagnosis; Doppler; Invasive.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: C.M.C. has received grants or research support from Edwards Lifesciences, honoraria or consultation fees from Boston Scientific, Philips, Viz.ai, and Medtronic and is a shareholder of Cerebria.ai and Viz.ai. S.N. has received honoraria for speaking on Coronary Physiology from Phillips. H.S. has received educational funding from Amgen. R.A.-L. has received speaking fees from Philips Volcano. R.P. has acted as consultant to Philips. T.P.v.d.H. has served as a speaker at educational events organized by Philips Volcano, St Jude Medical (now Abbott), and Boston Scientific. S.S. reports speaking fees for Philips, Pfizer, and Astra Zenenca and an Educational Grant from Medtronic. N.V.R. reports grants from Philips, Abbott, and Biotronik, and personal fees from Medtronic. All other authors have no conflicts to disclose.
Figures
Similar articles
-
Comparison of Doppler Flow Velocity and Thermodilution Derived Indexes of Coronary Physiology.JACC Cardiovasc Interv. 2022 May 23;15(10):1060-1070. doi: 10.1016/j.jcin.2022.03.015. JACC Cardiovasc Interv. 2022. PMID: 35589236 Free PMC article.
-
Assessment of flow velocity reserve by transthoracic Doppler echocardiography and venous adenosine infusion before and after left anterior descending coronary artery stenting.J Am Coll Cardiol. 2001 Jul;38(1):155-62. doi: 10.1016/s0735-1097(01)01333-x. J Am Coll Cardiol. 2001. PMID: 11451266
-
Regional myocardial perfusion reserve determined using myocardial perfusion magnetic resonance imaging showed a direct correlation with coronary flow velocity reserve by Doppler flow wire.Eur Heart J. 2009 Feb;30(4):444-52. doi: 10.1093/eurheartj/ehn521. Epub 2008 Dec 19. Eur Heart J. 2009. PMID: 19098020
-
What can intracoronary pressure measurements tell us about flow reserve? Pressure-Bounded coronary flow reserve and example application to the randomized DEFER trial.Catheter Cardiovasc Interv. 2017 Nov 15;90(6):917-925. doi: 10.1002/ccd.26972. Epub 2017 Mar 15. Catheter Cardiovasc Interv. 2017. PMID: 28296167 Review.
-
[Intravenous adenosine infusion in the assessment of coronary flow reserve in hypertension. Transesophageal Doppler echocardiographic study].Orv Hetil. 1999 Mar 7;140(10):523-7. Orv Hetil. 1999. PMID: 10323067 Review. Hungarian.
Cited by
-
Do You See the Writing on the Wall?: What Coronary Arteries Tell About Ventricular Function.JACC Adv. 2023 Oct 10;2(9):100631. doi: 10.1016/j.jacadv.2023.100631. eCollection 2023 Nov. JACC Adv. 2023. PMID: 38938719 Free PMC article.
-
A Comprehensive Literature Review Discussing Diagnostic Challenges of Prinzmetal or Vasospastic Angina.Cureus. 2025 May 8;17(5):e83745. doi: 10.7759/cureus.83745. eCollection 2025 May. Cureus. 2025. PMID: 40486459 Free PMC article. Review.
References
-
- Shimokawa H, Suda A, Takahashi J, Berry C, Camici PG, Crea F, et al. . Clinical characteristics and prognosis of patients with microvascular angina: an international and prospective cohort study by the Coronary Vasomotor Disorders International Study (COVADIS) group. Eur Heart J 2021;42:4592–4600. - PMC - PubMed
-
- Heggie R, Briggs A, Stanley B, Good R, Rocchiccioli P, McEntegart M, et al. . Stratified medicine using invasive coronary function testing in angina: a cost-effectiveness analysis of the British Heart Foundation CorMicA trial. Int J Cardiol 2021;337:44–51. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources