

Consultation on UTUC II Stockholm 2022: diagnostics, prognostication, and follow-up-where are we today?
- PMID: 37540248
- PMCID: PMC10693525
- DOI: 10.1007/s00345-023-04530-9
Consultation on UTUC II Stockholm 2022: diagnostics, prognostication, and follow-up-where are we today?
Abstract
Purpose: To summarise the current knowledge regarding diagnostics, prognostication and follow-up in upper tract urothelial carcinoma (UTUC).
Methods: A scoping review combined with expert opinion was applied to provide an overview of the current research field. Based on the published literature and the experts' own experience and opinions, consensus was reached through presentations and discussions at the meeting Consultation on UTUC II in Stockholm 2022.
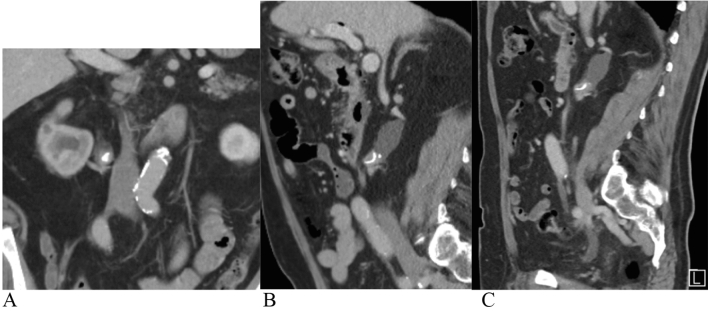
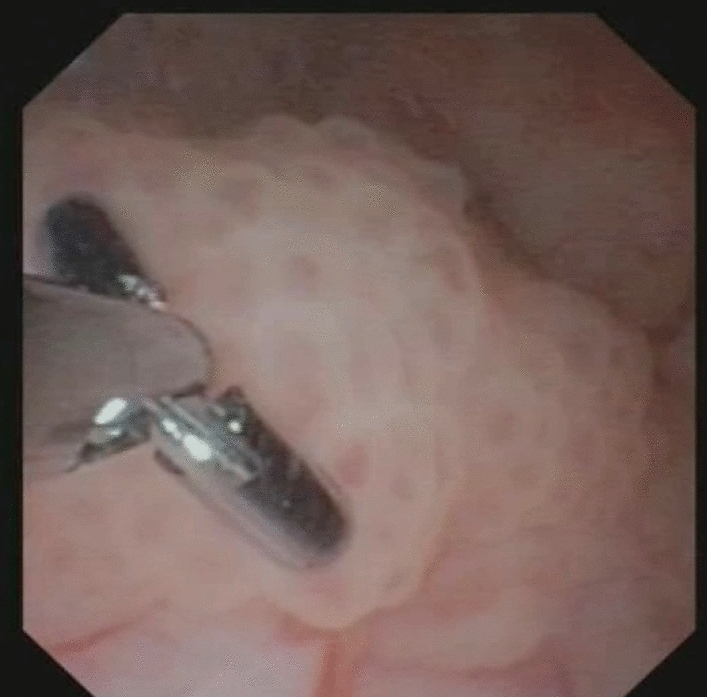
Results: The strongest prognostic factors in UTUC are tumour grade and stage. They are correlated, and grade is used for indirect staging. The diagnostic examinations should include multiphase computed tomography urography (CTU) with corticomedullary phase, and urethrocystoscopy with cytology. If there is no clear diagnosis for clinical decision-making, ureterorenoscopy (URS) with focal cytology and biopsies should be performed. Both WHO classification systems (1973/1999 and 2004/2016) should be used. Novel biomarker tests are not yet widespread nor recommended for the detection of UTUC. Long-term, regular follow-up, including URS in patients who have had organ-sparing treatment, is important to check for tumour recurrences, intravesical recurrences, metastases and progression of the tumour.
Conclusion: Proper diagnostics with correct grading of UTUC are necessary for appropriate treatment decisions. The diagnostics should include CTU with corticomedullary phase, urine or bladder cytology, URS with focal barbotage cytology, and biopsies when needed for proper diagnosis and risk stratification. Regular, long-term follow-ups are fundamental, due to the high rate of recurrence and risk of progression.
Keywords: Biopsy; Computed tomography urography; Cytology; Diagnostics; Follow-up; Prognostication; UTUC; Upper tract urothelial carcinoma; Ureterorenoscopy.
© 2023. The Author(s).
Conflict of interest statement
Filip Sydén: no conflict of interest; Joyce Baard: consultation for Coloplast, BSC, Urogen, and Olympus; Matthew Bultitude: no conflict of interest; Francis Xavier Keeley, Jr: no conflict of interest; Morgan Rouprêt: Advisory Board for Ferring, Roche, BMS, Janssen, Ipsen, and Bayer; Kay Thomas: no conflict of interest; Tómas Andri Axelsson: no conflict of interest; Georg Jaremko: no conflict of interest; Helene Jung: consultation for Boston Scientific and AMBU A/S; Camilla Malm: no conflict of interest; Silvia Proietti: no conflict of interest; Palle Jørn Sloth Osther: no conflict of interest; Marianne Brehmer: consultation for Boston Scientific.
Figures
References
-
- Li WM, Shen JT, Li CC, Ke HL, Wei YC, Wu WJ, et al. Oncologic outcomes following three different approaches to the distal ureter and bladder cuff in nephroureterectomy for primary upper urinary tract urothelial carcinoma. Eur Urol. 2010;57(6):963–969. doi: 10.1016/j.eururo.2009.12.032. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
