The ptotic tongue-imaging appearance and pathology localization along the course of the hypoglossal nerve
- PMID: 37540288
- PMCID: PMC10497427
- DOI: 10.1007/s00234-023-03204-y
The ptotic tongue-imaging appearance and pathology localization along the course of the hypoglossal nerve
Abstract
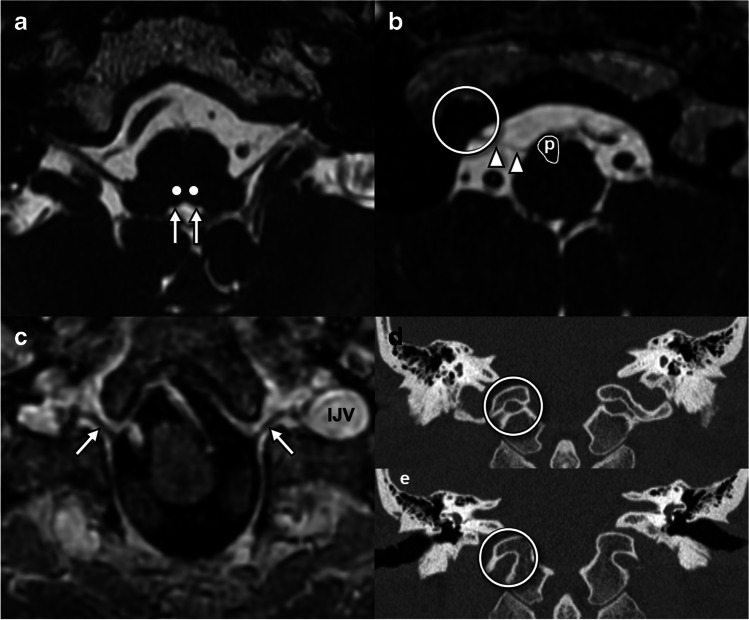
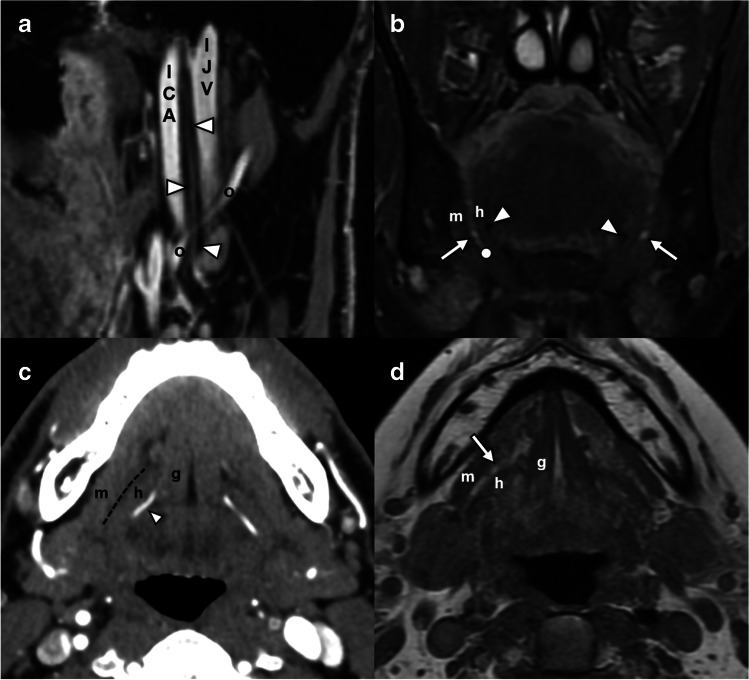
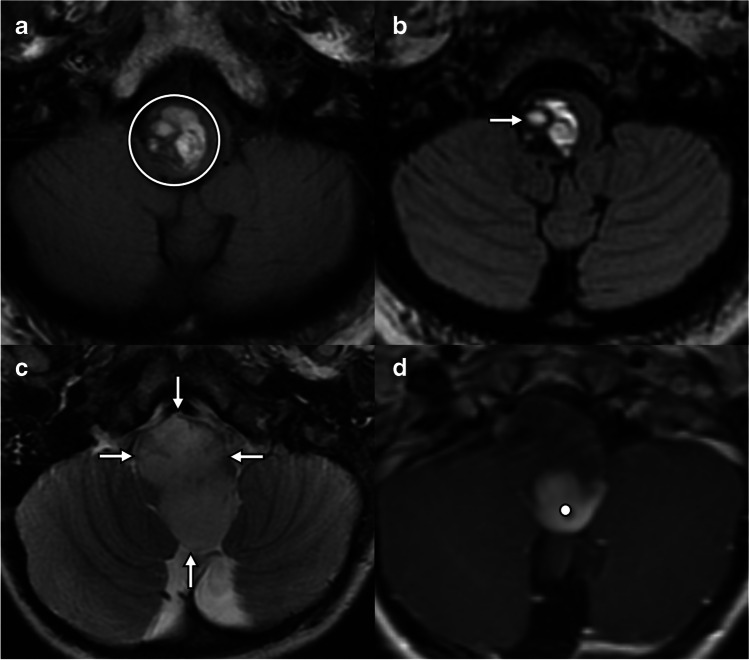
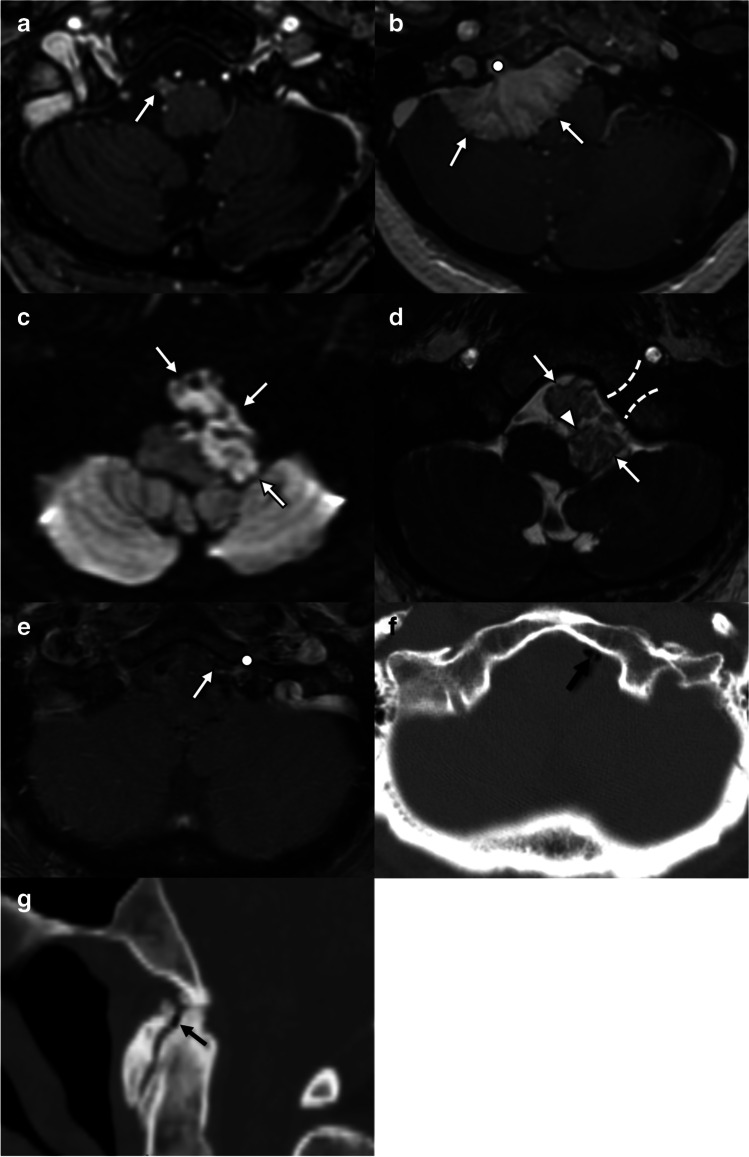
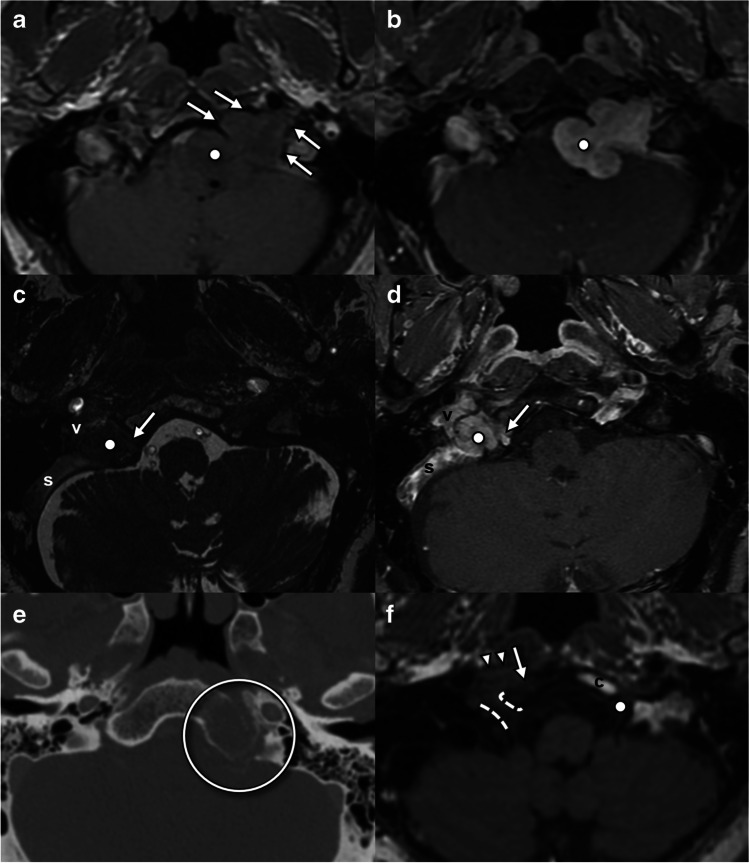
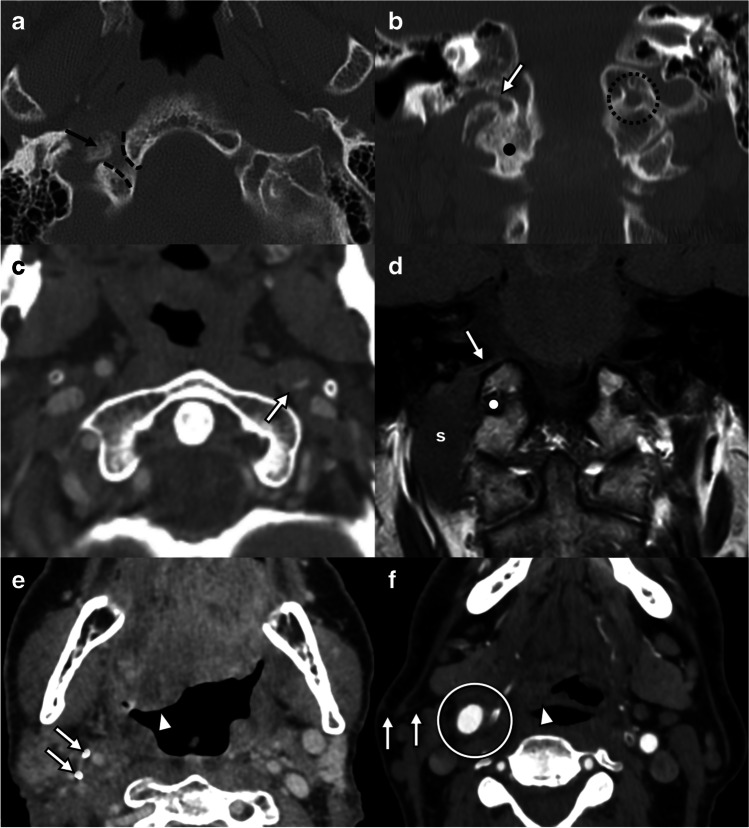
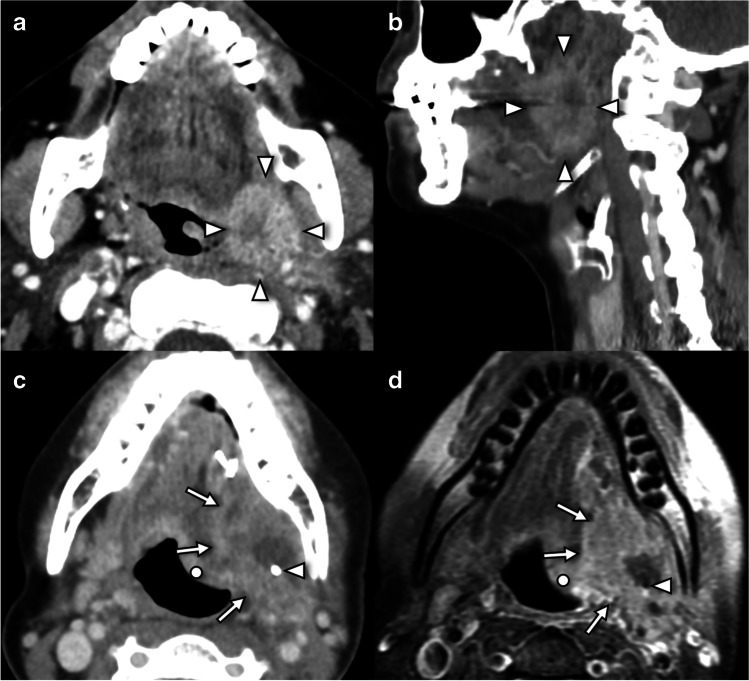
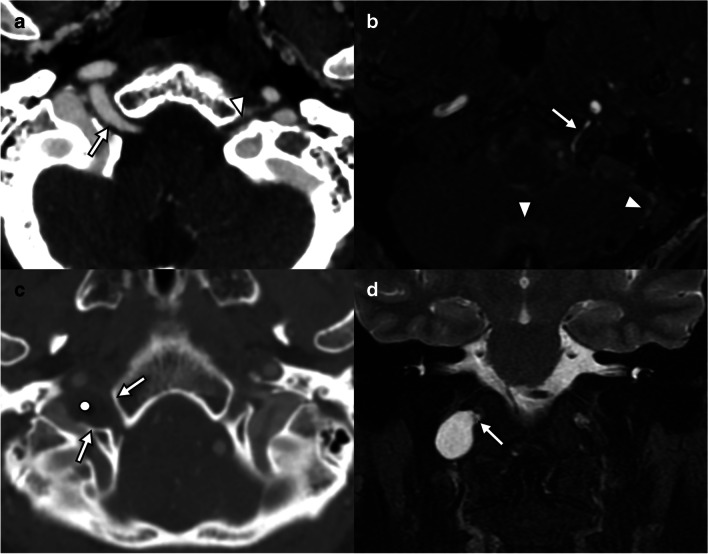
CT and MRI findings of tongue ptosis and atrophy should alert radiologists to potential pathology along the course of the hypoglossal nerve (cranial nerve XII), a purely motor cranial nerve which supplies the intrinsic and extrinsic muscles of the tongue. While relatively specific for hypoglossal nerve pathology, these findings do not accurately localize the site or cause of denervation. A detailed understanding of the anatomic extent of the nerve, which crosses multiple anatomic spaces, is essential to identify possible underlying pathology, which ranges from benign postoperative changes to life-threatening medical emergencies. This review will describe key imaging findings of tongue denervation, segmental anatomy of the hypoglossal nerve, imaging optimization, and comprehensive imaging examples of diverse pathology which may affect the hypoglossal nerve. Armed with this knowledge, radiologists will increase their sensitivity for detection of pathology and provide clinically relevant differential diagnoses when faced with findings of tongue ptosis and denervation.
Keywords: Denervation; Hypoglossal; Hypoglossal palsy; MRI; Ptosis.
© 2023. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures