

Left-sided valvular heart disease and survival in out-of-hospital cardiac arrest: a nationwide registry-based study
- PMID: 37542095
- PMCID: PMC10403503
- DOI: 10.1038/s41598-023-39570-z
Left-sided valvular heart disease and survival in out-of-hospital cardiac arrest: a nationwide registry-based study
Abstract
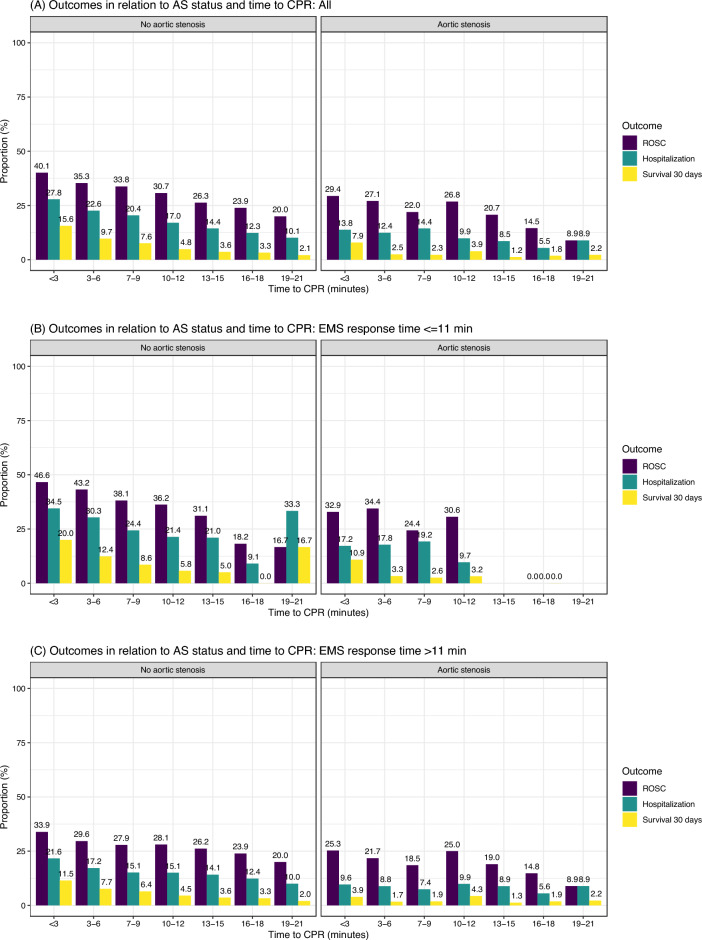
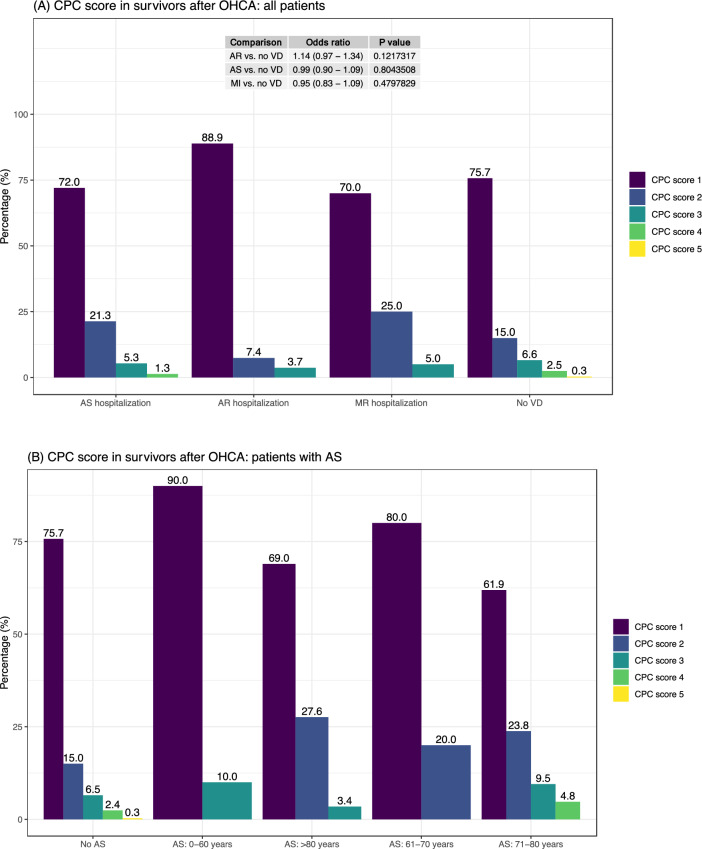
Survival in left-sided valvular heart disease (VHD; aortic stenosis [AS], aortic regurgitation [AR], mitral stenosis [MS], mitral regurgitation [MR]) in out-of-hospital cardiac arrest (OHCA) is unknown. We studied all cases of OHCA in the Swedish Registry for Cardiopulmonary Resuscitation. All degrees of VHD, diagnosed prior to OHCA, were included. Association between VHD and survival was studied using logistic regression, gradient boosting and Cox regression. We studied time to cardiac arrest, comorbidities, survival, and cerebral performance category (CPC) score. We included 55,615 patients; 1948 with AS (3,5%), 384 AR (0,7%), 17 MS (0,03%), and 704 with MR (1,3%). Patients with MS were not described due to low case number. Time from VHD diagnosis to cardiac arrest was 3.7 years in AS, 4.5 years in AR and 4.1 years in MR. ROSC occurred in 28% with AS, 33% with AR, 36% with MR and 35% without VHD. Survival at 30 days was 5.2%, 10.4%, 9.2%, 11.4% in AS, AR, MR and without VHD, respectively. There were no survivors in people with AS presenting with asystole or PEA. CPC scores did not differ in those with VHD compared with no VHD. Odds ratio (OR) for MR and AR showed no difference in survival, while AS displayed OR 0.58 (95% CI 0.46-0.72), vs no VHD. AS is associated with halved survival in OHCA, while AR and MR do not affect survival. Survivors with AS have neurological outcomes comparable to patients without VHD.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Otto CM, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. 2021;143:e72–e227. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
