

Radiotherapy plus anti-PD1 versus radiotherapy for hepatic toxicity in patients with hepatocellular carcinoma
- PMID: 37542246
- PMCID: PMC10403970
- DOI: 10.1186/s13014-023-02309-1
Radiotherapy plus anti-PD1 versus radiotherapy for hepatic toxicity in patients with hepatocellular carcinoma
Abstract
Purpose: In this study, we aimed to compare the radiation-induced hepatic toxicity (RIHT) outcomes of radiotherapy (RT) plus antibodies against programmed cell death protein 1 (anti-PD1) versus RT alone in patients with hepatocellular carcinoma (HCC), evaluate prognostic factors of non-classic radiation-induced liver disease (ncRILD), and establish a nomogram for predicting the probability of ncRILD.
Patients and methods: Patients with unresectable HCC treated with RT and anti-PD1 (RT + PD1, n = 30) or RT alone (n = 66) were enrolled retrospectively. Patients (n = 30) in each group were placed in a matched cohort using propensity score matching (PSM). Treatment-related hepatotoxicity was evaluated and analyzed before and after PSM. The prognostic factors affecting ncRILD were identified by univariable logistic analysis and Spearman's rank test in the matched cohort to generate a nomogram.
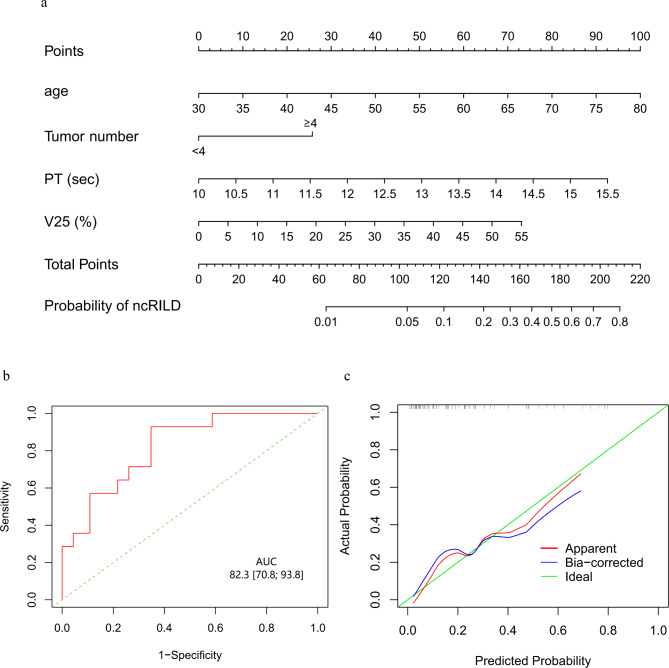
Results: There were no differences in RIHT except for increased aspartate aminotransferase (AST) ≥ grade 1 and increased total bilirubin ≥ grade 1 between the two groups before PSM. After PSM, AST ≥ grade 1 occurred more frequently in the RT + PD1 group (p = 0.020), and there were no significant differences in other hepatotoxicity metrics between the two groups. In the matched cohort, V25, tumor number, age, and prothrombin time (PT) were the optimal prognostic factors for ncRILD modeling. A nomogram revealed a good predictive performance (area under the curve = 0.82).
Conclusions: The incidence of RIHT in patients with HCC treated with RT + PD1 was acceptable and similar to that of RT treatment. The nomogram based on V25, tumor number, age, and PT robustly predicted the probability of ncRILD.
Keywords: Anti-PD1; Hepatocellular carcinoma; Propensity score matching; Radiation-induced liver disease.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Non-classic radiation-induced liver disease after intensity-modulated radiotherapy for Child-Pugh grade B patients with locally advanced hepatocellular carcinoma.Radiat Oncol. 2023 Mar 8;18(1):48. doi: 10.1186/s13014-023-02232-5. Radiat Oncol. 2023. PMID: 36890592 Free PMC article.
-
Radiotherapy enhances efficacy of PD-1 inhibitors in advanced hepatocellular carcinoma: A propensity-matched real-world study.Chin Med J (Engl). 2024 Jun 5;137(11):1332-1342. doi: 10.1097/CM9.0000000000003124. Epub 2024 May 9. Chin Med J (Engl). 2024. PMID: 38725345 Free PMC article.
-
Efficacy and safety of radiotherapy plus anti-PD1 versus transcatheter arterial chemoembolization plus sorafenib for advanced hepatocellular carcinoma: a real-world study.Radiat Oncol. 2022 Jun 11;17(1):106. doi: 10.1186/s13014-022-02075-6. Radiat Oncol. 2022. PMID: 35690773 Free PMC article.
-
A Novel Nomogram to Predict Prognosis of Advanced Hepatocellular Carcinoma Treated with Intensity-Modulated Radiotherapy Plus Anti-PD1.J Hepatocell Carcinoma. 2024 May 22;11:913-925. doi: 10.2147/JHC.S459683. eCollection 2024. J Hepatocell Carcinoma. 2024. PMID: 38799002 Free PMC article.
-
Radiation-induced hypothyroidism after treatment of head and neck cancer.Dan Med J. 2016 Mar;63(3):B5213. Dan Med J. 2016. PMID: 26931197 Review.
Cited by
-
Safety and toxicity risks of radiotherapy combined with PD-1/PD-L1 inhibitors: A comprehensive review.iScience. 2025 Jun 27;28(7):112882. doi: 10.1016/j.isci.2025.112882. eCollection 2025 Jul 18. iScience. 2025. PMID: 40697412 Free PMC article. Review.
-
Risk Factors of Non-Classic Radiation-Induced Liver Disease (ncRILD) After Intensity-Modulated Radiotherapy in Hepatocellular Carcinoma.Cancer Manag Res. 2025 Jun 18;17:1169-1183. doi: 10.2147/CMAR.S539527. eCollection 2025. Cancer Manag Res. 2025. PMID: 40546439 Free PMC article.
-
Prognostic nomogram of overall survival for radiation therapy in hepatocellular carcinoma: a population study based on the SEER database and an external cohort.Front Oncol. 2024 Sep 2;14:1371409. doi: 10.3389/fonc.2024.1371409. eCollection 2024. Front Oncol. 2024. PMID: 39286027 Free PMC article.
-
Treatment of intermediate-to-advanced unresectable hepatocellular carcinoma is shifting toward a multidisciplinary strategy that includes multiple modalities as needed.World J Gastroenterol. 2025 Mar 14;31(10):103420. doi: 10.3748/wjg.v31.i10.103420. World J Gastroenterol. 2025. PMID: 40093678 Free PMC article.
-
Radiomics of Dynamic Contrast-Enhanced MRI for Predicting Radiation-Induced Hepatic Toxicity After Intensity Modulated Radiotherapy for Hepatocellular Carcinoma: A Machine Learning Predictive Model Based on the SHAP Methodology.J Hepatocell Carcinoma. 2025 May 17;12:999-1015. doi: 10.2147/JHC.S523448. eCollection 2025. J Hepatocell Carcinoma. 2025. PMID: 40406666 Free PMC article.
References
MeSH terms
Substances
Grants and funding
- AA18221001/Key Research and Development Project of Guangxi
- S2019039/Development and Application Project for the Appropriate Technology of Health of Guangxi Province
- Z20201371/Self-Raised Scientific Research Fund of the Ministry of Health of Guangxi Province
- 2021-10/Youth Program of Scientific Research Foundation of Guangxi Medical University Cancer Hospital
- 2022KY0079/Guangxi Universities Training Program of Young Teachers
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
