

Spatial tumour gene signature discriminates neoplastic from non-neoplastic compartments in colon cancer: unravelling predictive biomarkers for relapse
- PMID: 37543577
- PMCID: PMC10403907
- DOI: 10.1186/s12967-023-04384-0
Spatial tumour gene signature discriminates neoplastic from non-neoplastic compartments in colon cancer: unravelling predictive biomarkers for relapse
Abstract
Background: Opting for or against the administration of adjuvant chemotherapy in therapeutic management of stage II colon cancer remains challenging. Several studies report few survival benefits for patients treated with adjuvant therapy and additionally revealing potential side effects of overtreatment, including unnecessary exposure to chemotherapy-induced toxicities and reduced quality of life. Predictive biomarkers are urgently needed. We, therefore, hypothesise that the spatial tissue composition of relapsed and non-relapsed colon cancer stage II patients reveals relevant biomarkers.
Methods: The spatial tissue composition of stage II colon cancer patients was examined by a novel spatial transcriptomics technology with sub-cellular resolution, namely in situ sequencing. A panel of 176 genes investigating specific cancer-associated processes such as apoptosis, proliferation, angiogenesis, stemness, oxidative stress, hypoxia, invasion and components of the tumour microenvironment was designed to examine differentially expressed genes in tissue of relapsed versus non-relapsed patients. Therefore, FFPE slides of 10 colon cancer stage II patients either classified as relapsed (5 patients) or non-relapsed (5 patients) were in situ sequenced and computationally analysed.
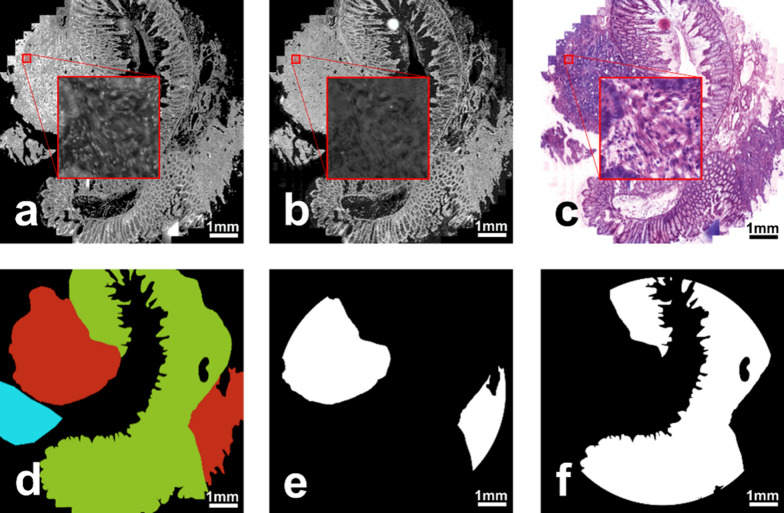
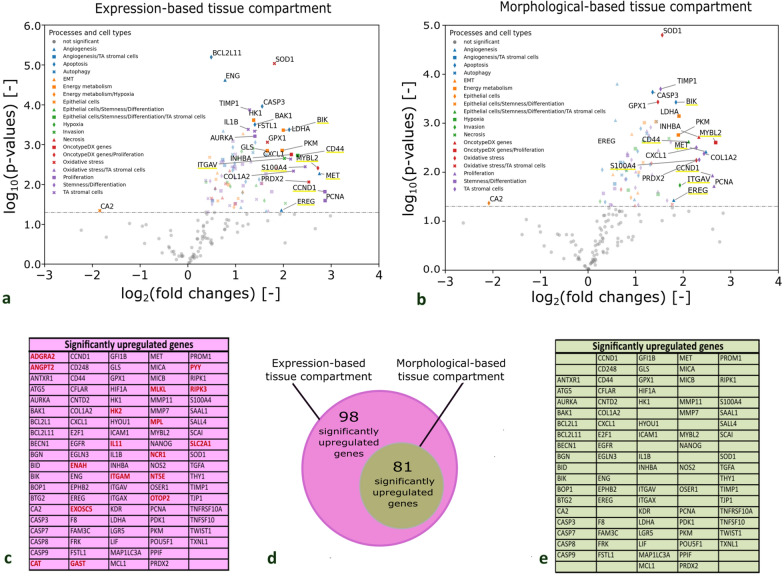
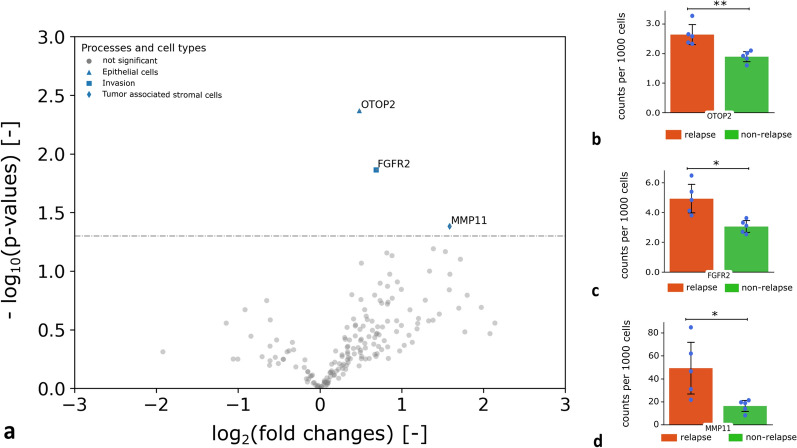
Results: We identified a tumour gene signature that enables the subclassification of tissue into neoplastic and non-neoplastic compartments based on spatial expression patterns obtained through in situ sequencing. We developed a computational tool called Genes-To-Count (GTC), which automates the quantification of in situ signals, accurately mapping their position onto the spatial tissue map and automatically identifies neoplastic and non-neoplastic tissue compartments. The GTC tool was used to quantify gene expression of biological processes upregulated within the neoplastic tissue in comparison to non-neoplastic tissue and within relapsed versus non-relapsed stage II colon patients. Three differentially expressed genes (FGFR2, MMP11 and OTOP2) in the neoplastic tissue compartments of relapsed patients in comparison to non-relapsed patients were identified predicting recurrence in stage II colon cancer.
Conclusions: In depth spatial in situ sequencing showed potential to provide a deeper understanding of the underlying mechanisms involved in the recurrence of disease and revealed novel potential predictive biomarkers for disease relapse in colon cancer stage II patients. Our open-access GTC-tool allowed us to accurately capture the tumour compartment and quantify spatial gene expression in colon cancer tissue.
Keywords: In situ sequencing; Predictive biomarker; Spatial transcriptomics; Tumour compartment; Tumour gene signature; colon cancer.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
No competing interests must be declared.
Figures



References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
