

Pathophysiology, clinical presentation, and management of ketamine-induced cystitis
- PMID: 37545795
- PMCID: PMC10399845
- DOI: 10.4103/tcmj.tcmj_94_23
Pathophysiology, clinical presentation, and management of ketamine-induced cystitis
Abstract
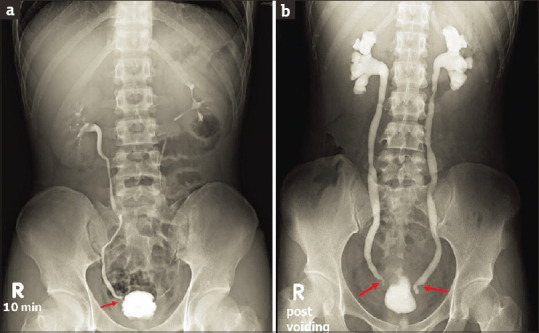
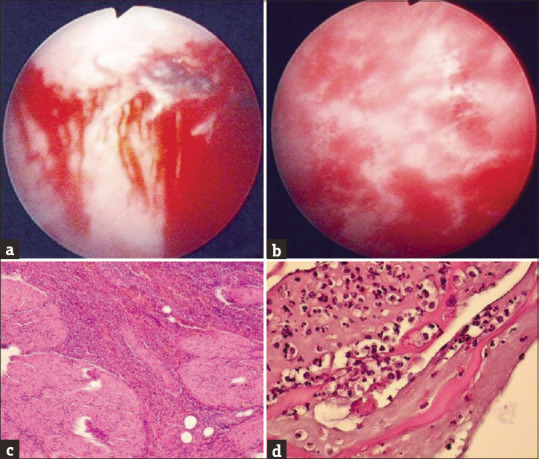
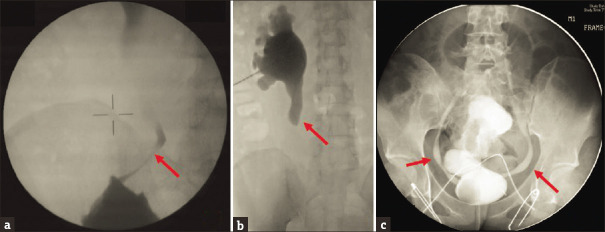
Ketamine is illegally used as a recreational drug in many Asian countries. Long-term ketamine abusers often develop irritable bladder symptoms that gradually develop into more severe urinary frequency and urgency and eventually into a painful ulcerated bladder. These patients typically have reduced functional bladder capacity, increased bladder sensation, detrusor overactivity, severe urgency, urinary incontinence, and bladder contracture. Ketamine metabolites can cause severe inflammation of the urothelium, urothelial barrier deficits, vascular endothelial fibrinoid changes, increased oxidative stress, and bladder wall fibrosis. A decrease in bladder compliance, urinary tract infection, severe bladder pain with a full bladder, and painful micturition are also common symptoms. Finally, with continued abuse of ketamine, hydronephrosis, ureteral stricture, vesicoureteral reflux, and renal failure may develop. Cessation of ketamine is the mainstay of treatment. Lower urinary tract symptoms usually relapse if patients reuse ketamine after stopping. In cases of severe ketamine cystitis, only augmentation enterocystoplasty can relieve bladder pain and restore normal lower urinary tract function. This article reviews the underlying pathophysiology, clinical characteristics, and management of ketamine cystitis.
Keywords: Augmentation; contracted bladder; cystitis; ketamine; treatment.
Copyright: © 2023 Tzu Chi Medical Journal.
Conflict of interest statement
Dr. Hann-Chorng Kuo, the editorial board member at Tzu Chi Medical Journal, played no role in the peer review process or decision to publish this article. The other authors declared no conflicts of interest in writing this paper.
Figures




References
-
- Shahani R, Streutker C, Dickson B, Stewart RJ. Ketamine-associated ulcerative cystitis:A new clinical entity. Urology. 2007;69:810–2. - PubMed
-
- Chu PS, Ma WK, Wong SC, Chu RW, Cheng CH, Wong S, et al. The destruction of the lower urinary tract by ketamine abuse:A new syndrome? BJU Int. 2008;102:1616–22. - PubMed
-
- Recreational Ketamine Use Has Increased in Recent Years, But Remains Rare. [Last accessed on 2023 Apr 16]. Available from:https://www.nyu.edu/about/news-publications/news/2021/october/recreation... .
-
- Chen CH, Lee MH, Chen YC, Lin MF. Ketamine-snorting associated cystitis. J Formos Med Assoc. 2011;110:787–91. - PubMed
LinkOut - more resources
Full Text Sources