

A multiphysics model to predict periventricular white matter hyperintensity growth during healthy brain aging
- PMID: 37546181
- PMCID: PMC10399513
- DOI: 10.1016/j.brain.2023.100072
A multiphysics model to predict periventricular white matter hyperintensity growth during healthy brain aging
Abstract
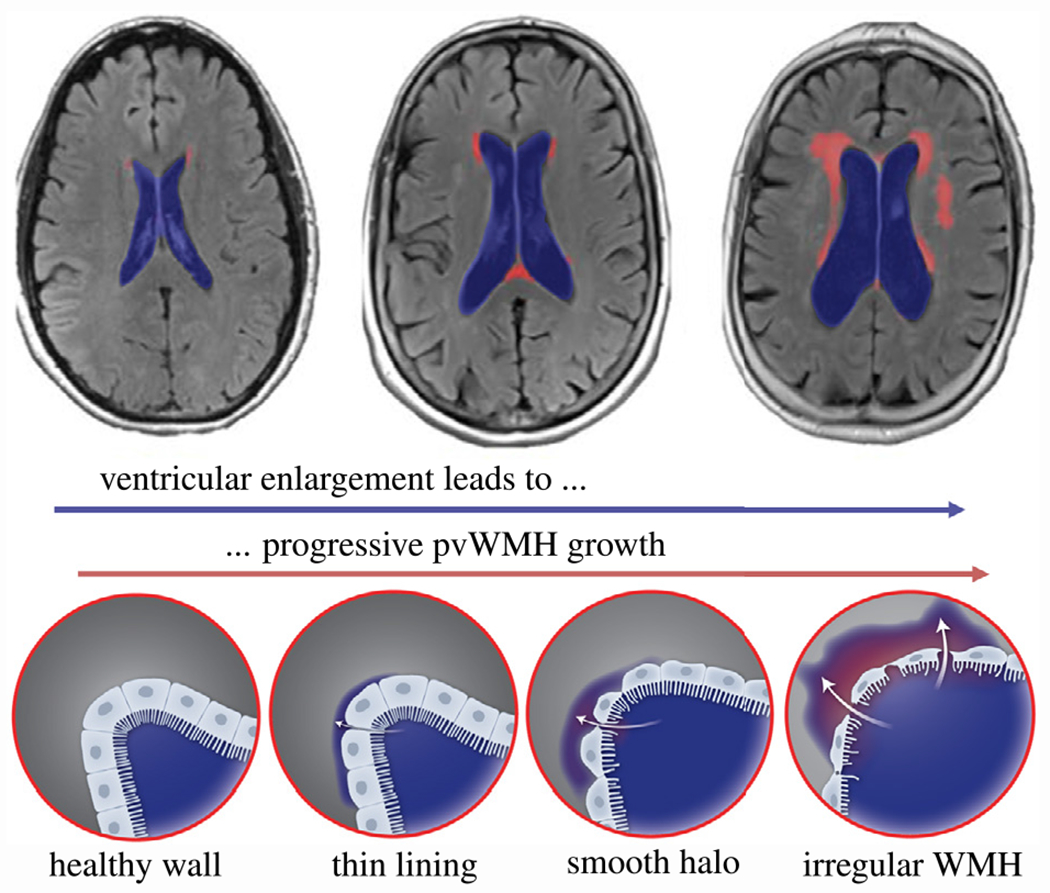
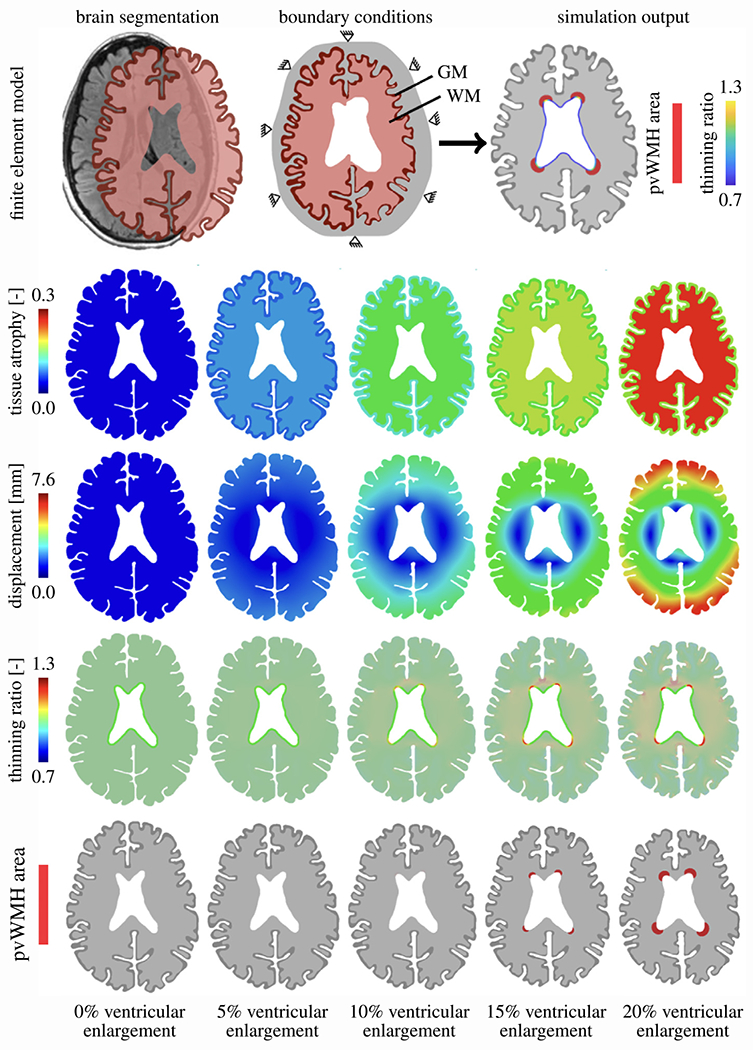
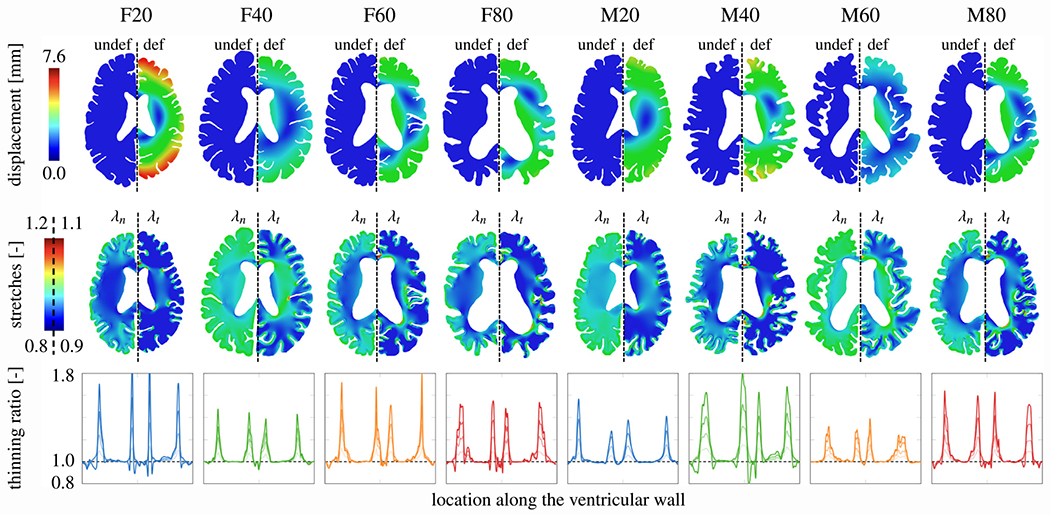
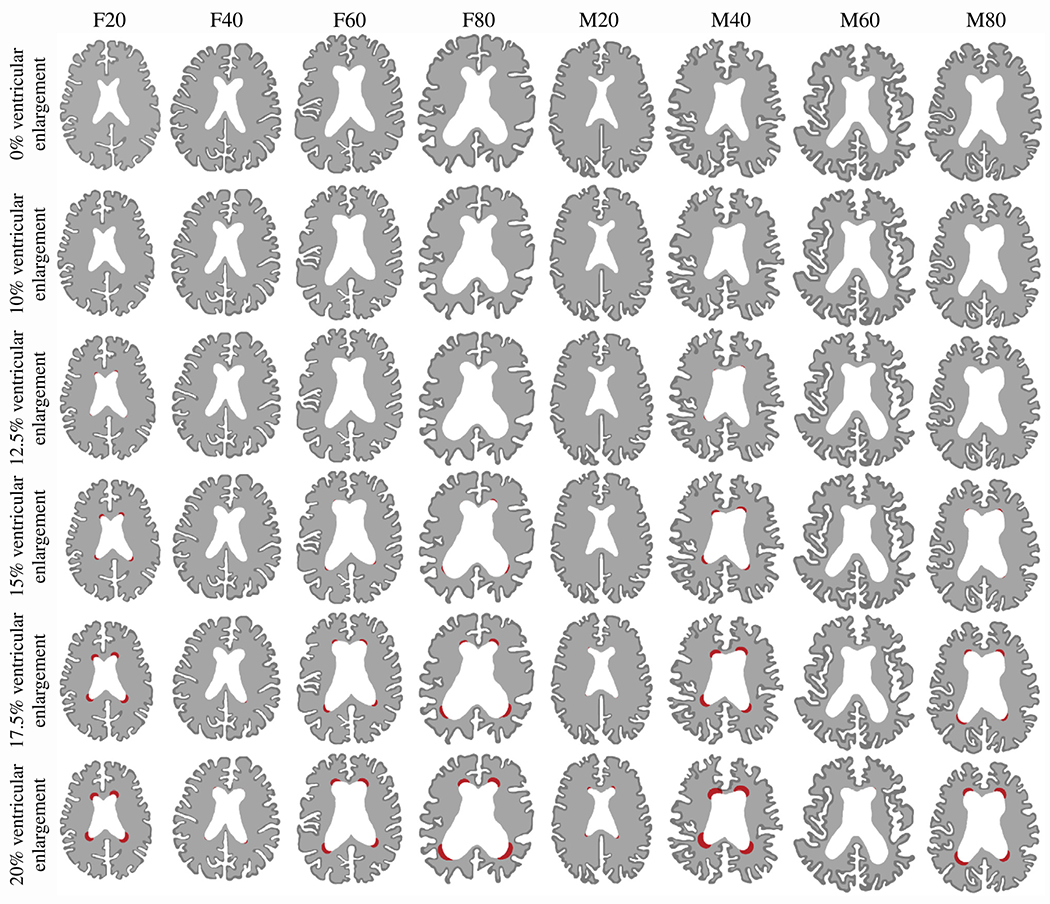
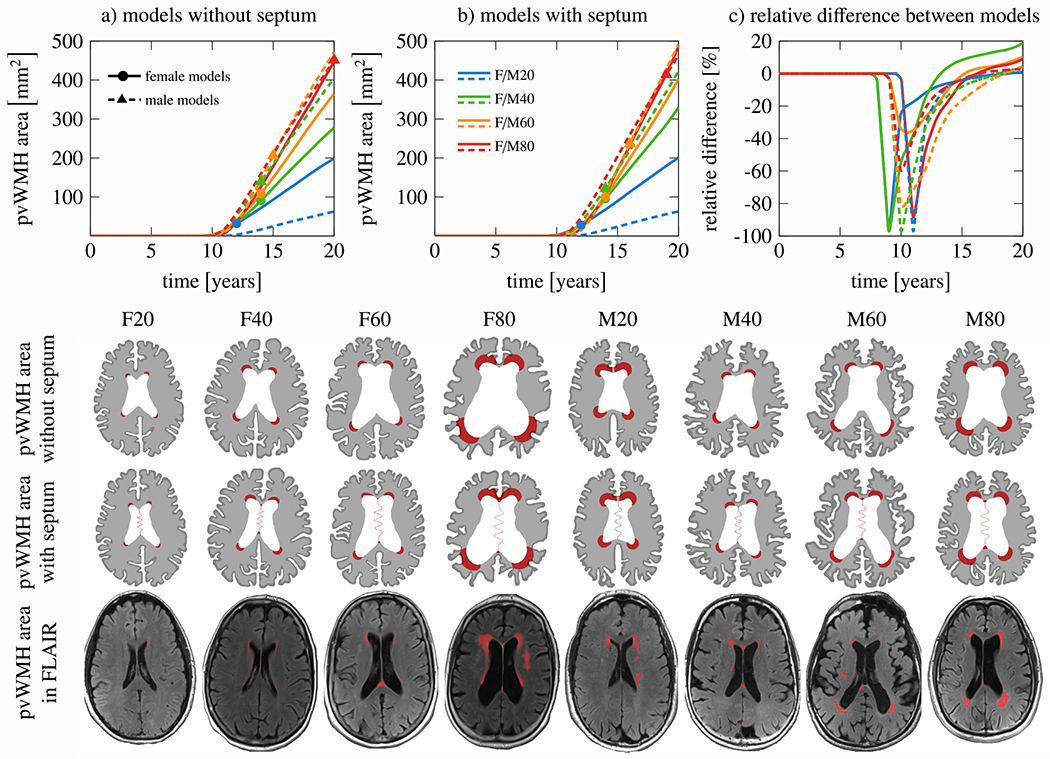
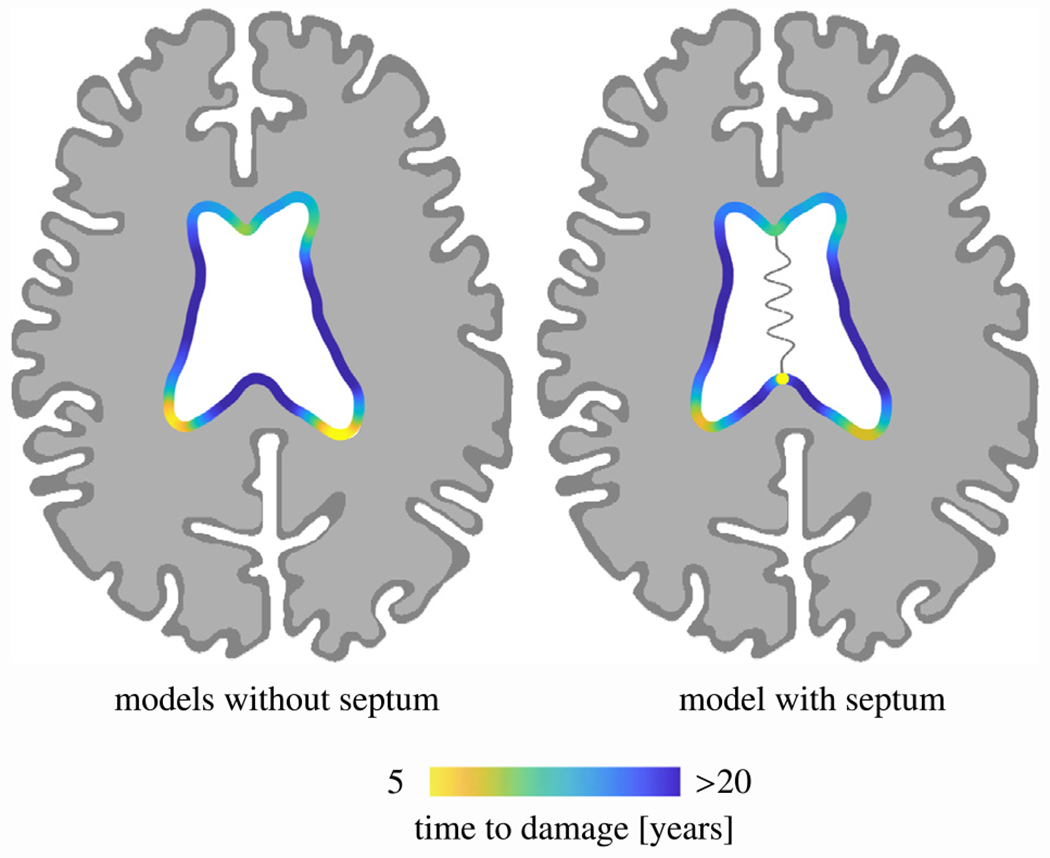
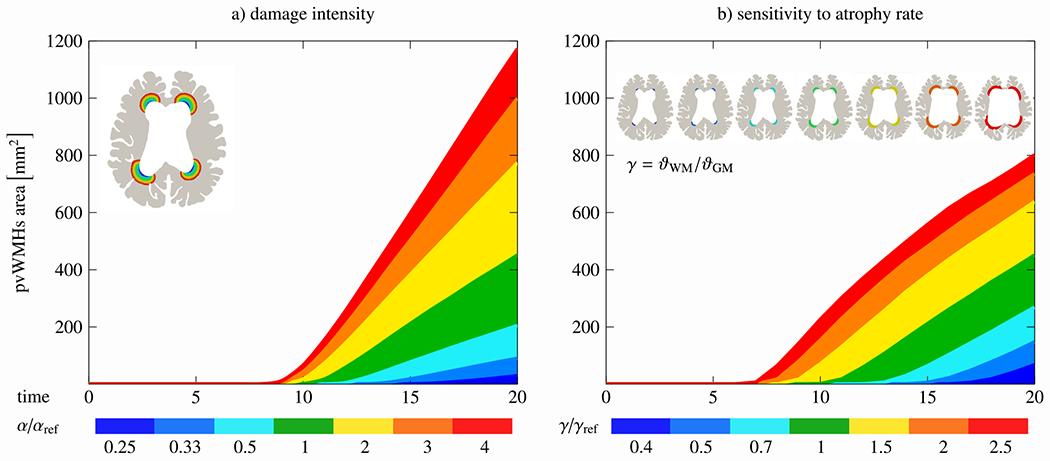
Periventricular white matter hyperintensities (WMH) are a common finding in medical images of the aging brain and are associated with white matter damage resulting from cerebral small vessel disease, white matter inflammation, and a degeneration of the lateral ventricular wall. Despite extensive work, the etiology of periventricular WMHs remains unclear. We pose that there is a strong coupling between age-related ventricular expansion and the degeneration of the ventricular wall which leads to a dysregulated fluid exchange across this brain-fluid barrier. Here, we present a multiphysics model that couples cerebral atrophy-driven ventricular wall loading with periventricular WMH formation and progression. We use patient data to create eight 2D finite element models and demonstrate the predictive capabilities of our damage model. Our simulations show that we accurately capture the spatiotemporal features of periventricular WMH growth. For one, we observe that damage appears first in both the anterior and posterior horns and then spreads into deeper white matter tissue. For the other, we note that it takes up to 12 years before periventricular WMHs first appear and derive an average annualized periventricular WMH damage growth rate of 15.2 ± 12.7 mm2/year across our models. A sensitivity analysis demonstrated that our model parameters provide sufficient sensitivity to rationalize subject-specific differences with respect to onset time and damage growth. Moreover, we show that the septum pellucidum, a membrane that separates the left and right lateral ventricles, delays the onset of periventricular WMHs at first, but leads to a higher WMH load in the long-term.
Keywords: Finite element modeling; Multiphysics damage model; Periventricular white matter hyperintensities; Ventricular wall loading.
Figures
Similar articles
-
Mechanical loading of the ventricular wall as a spatial indicator for periventricular white matter degeneration.J Mech Behav Biomed Mater. 2023 Jul;143:105921. doi: 10.1016/j.jmbbm.2023.105921. Epub 2023 May 24. J Mech Behav Biomed Mater. 2023. PMID: 37269602 Free PMC article.
-
3D finite-element brain modeling of lateral ventricular wall loading to rationalize periventricular white matter hyperintensity locations.Eng Comput. 2022 Oct;38(5):3939-3955. doi: 10.1007/s00366-022-01700-y. Epub 2022 Jul 19. Eng Comput. 2022. PMID: 37485473 Free PMC article.
-
Longitudinal relaxographic imaging of white matter hyperintensities in the elderly.Fluids Barriers CNS. 2014 Oct 20;11:24. doi: 10.1186/2045-8118-11-24. eCollection 2014. Fluids Barriers CNS. 2014. PMID: 25379172 Free PMC article.
-
Peak ependymal cell stretch overlaps with the onset locations of periventricular white matter lesions.Sci Rep. 2021 Nov 9;11(1):21956. doi: 10.1038/s41598-021-00610-1. Sci Rep. 2021. PMID: 34753951 Free PMC article.
-
Associations Between White Matter Hyperintensity Burden, Cerebral Blood Flow and Transit Time in Small Vessel Disease: An Updated Meta-Analysis.Front Neurol. 2021 May 4;12:647848. doi: 10.3389/fneur.2021.647848. eCollection 2021. Front Neurol. 2021. PMID: 34017302 Free PMC article.
Cited by
-
Single-nucleus RNA sequencing of human periventricular white matter in vascular dementia.bioRxiv [Preprint]. 2024 Dec 10:2024.12.06.627202. doi: 10.1101/2024.12.06.627202. bioRxiv. 2024. PMID: 39713290 Free PMC article. Preprint.
-
White matter hyperintensities in dementia with lewy bodies and posterior cortical atrophy.Neurobiol Aging. 2025 Jun;150:44-52. doi: 10.1016/j.neurobiolaging.2025.03.002. Epub 2025 Mar 3. Neurobiol Aging. 2025. PMID: 40056539
References
-
- Wen W, Sachdev P, The topography of white matter hyperintensities on brain mri in healthy 60-to 64-year-old individuals, Neuroimage 22 (2004) 144–154. - PubMed
-
- Sachdev P, Wen W, Should we distinguish between periventricular and deep white matter hyperintensities? Stroke 36 (2005) 2342–2344. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources