

Diffuse alveolar hemorrhage after hematopoietic cell transplantation- response to treatments and risk factors for mortality
- PMID: 37546403
- PMCID: PMC10399223
- DOI: 10.3389/fonc.2023.1232621
Diffuse alveolar hemorrhage after hematopoietic cell transplantation- response to treatments and risk factors for mortality
Abstract
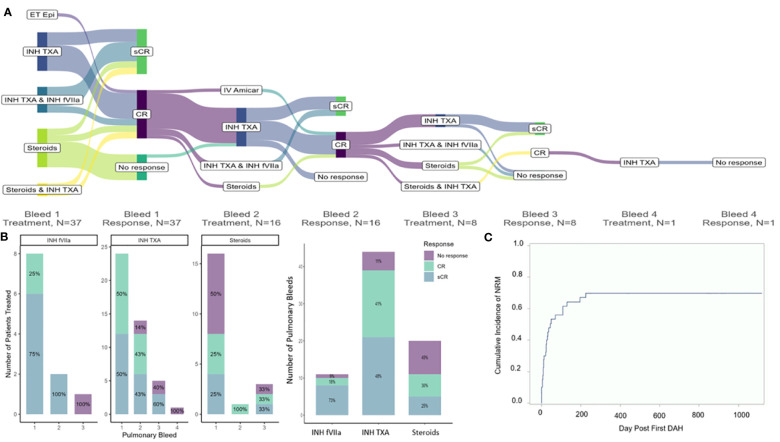
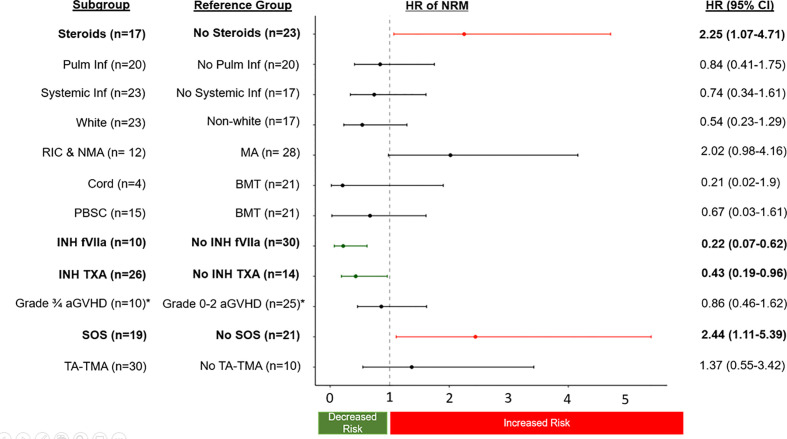
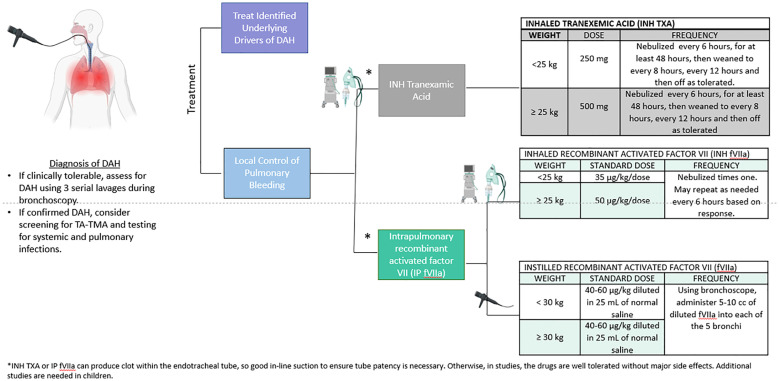
Diffuse alveolar hemorrhage (DAH) is a life-threatening complication of hematopoietic cellular therapy (HCT). This study aimed to evaluate the effect of DAH treatments on outcomes using data from consecutive HCT patients clinically diagnosed with DAH from 3 institutions between January 2018-August 2022. Endpoints included sustained complete response (sCR) defined as bleeding cessation without recurrent bleeding, and non-relapse mortality (NRM). Forty children developed DAH at a median of 56.5 days post-HCT (range 1-760). Thirty-five (88%) had at least one concurrent endothelial disorder, including transplant-associated thrombotic microangiopathy (n=30), sinusoidal obstructive syndrome (n=19), or acute graft versus host disease (n=10). Fifty percent had a concurrent pulmonary infection at the time of DAH. Common treatments included steroids (n=17, 25% sCR), inhaled tranexamic acid (INH TXA,n=26, 48% sCR), and inhaled recombinant activated factor VII (INH fVIIa, n=10, 73% sCR). NRM was 56% 100 days after first pulmonary bleed and 70% at 1 year. Steroid treatment was associated with increased risk of NRM (HR 2.25 95% CI 1.07-4.71, p=0.03), while treatment with INH TXA (HR 0.43, 95% CI 0.19- 0.96, p=0.04) and INH fVIIa (HR 0.22, 95% CI 0.07-0.62, p=0.005) were associated with decreased risk of NRM. Prospective studies are warranted to validate these findings.
Keywords: diffuse alveolar hemorrhage (DAH); inhaled recombinant activated factor VIIa (INH fVIIa); inhaled tranexamic acid (INH TXA); non-relapse related mortality; sinusoidal obstructive syndrome (SOS); steroids; transplant-associated thrombotic microangiopathy (TA-TMA).
Copyright © 2023 Schoettler, Dandoy, Harris, Chan, Tarquinio, Jodele, Qayed, Watkins, Kamat, Petrillo, Obordo, Higham, Dvorak, Westbrook, Zinter and Williams.
Conflict of interest statement
MS is a consultant for Alexion and Omeros. MZ is a consultant for Sobi. CCD is a consultant for Alexion and Jazz. CH is a consultant for Omeros. MQ has honorarium from Novartis and Vertex. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Wells J, Frankel SK. Alveolar hemorrhage. In: Cottin V, Cordier J-F, Richeldi L, editors. Orphan lung dis a clin guid to rare lung dis (2014) (Orphan Lung Diseases). p. 155–75. doi: 10.1007/978-1-4471-2401-6_10 - DOI
-
- Srivastava A, Gottlieb D, Bradstock KF. Diffuse alveolar haemorrhage associated with microangiopathy after allogeneic bone marrow transplantation. Bone Marrow Transpl (1995) 15(6):863–7. - PubMed