

This is a preprint.
Use of Electronic Health Records to Characterize Patients with Uncontrolled Hypertension in Two Large Health System Networks
- PMID: 37546792
- PMCID: PMC10402222
- DOI: 10.1101/2023.07.26.23293225
Use of Electronic Health Records to Characterize Patients with Uncontrolled Hypertension in Two Large Health System Networks
Update in
-
Use of electronic health records to characterize patients with uncontrolled hypertension in two large health system networks.BMC Cardiovasc Disord. 2024 Sep 18;24(1):497. doi: 10.1186/s12872-024-04161-x. BMC Cardiovasc Disord. 2024. PMID: 39289597 Free PMC article.
Abstract
Background: Improving hypertension control is a public health priority. However, uncertainty remains regarding the optimal way to identify patients with uncontrolled hypertension using electronic health records (EHR) data.
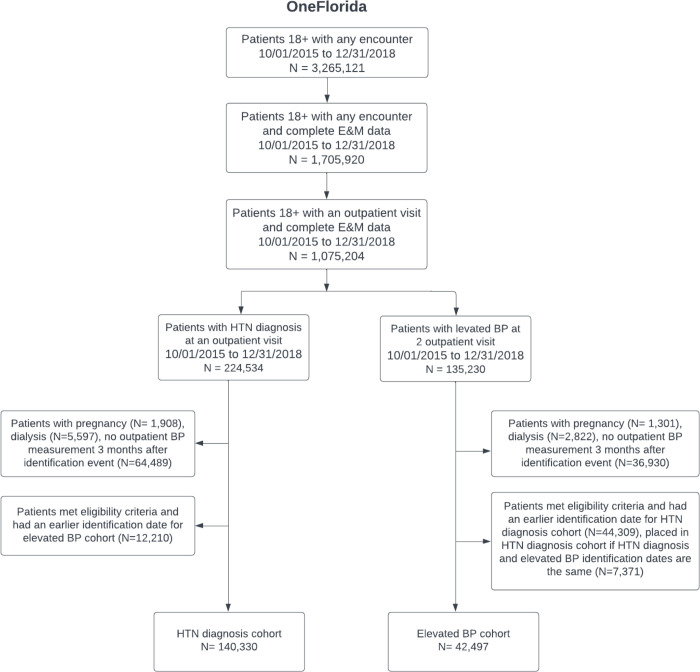
Methods: In this retrospective cohort study, we applied computable definitions to the EHR data to identify patients with controlled and uncontrolled hypertension and to evaluate differences in characteristics, treatment, and clinical outcomes between these patient populations. We included adult patients (≥18 years) with hypertension receiving ambulatory care within Yale-New Haven Health System (YNHHS; a large US health system) and OneFlorida Clinical Research Consortium (OneFlorida; a Clinical Research Network comprised of 16 health systems) between October 2015 and December 2018. We identified patients with controlled and uncontrolled hypertension based on either a single blood pressure (BP) measurement from a randomly selected visit or all BP measurements recorded between hypertension identification and the randomly selected visit).
Results: Overall, 253,207 and 182,827 adults at YNHHS and OneFlorida were identified as having hypertension. Of these patients, 83.1% at YNHHS and 76.8% at OneFlorida were identified using ICD-10-CM codes, whereas 16.9% and 23.2%, respectively, were identified using elevated BP measurements (≥ 140/90 mmHg). Uncontrolled hypertension was observed among 32.5% and 43.7% of patients at YNHHS and OneFlorida, respectively. Uncontrolled hypertension was disproportionately higher among Black patients when compared with White patients (38.9% versus 31.5% in YNHHS; p<0.001; 49.7% versus 41.2% in OneFlorida; p<0.001). Medication prescription for hypertension management was more common in patients with uncontrolled hypertension when compared with those with controlled hypertension (overall treatment rate: 39.3% versus 37.3% in YNHHS; p=0.04; 42.2% versus 34.8% in OneFlorida; p<0.001). Patients with controlled and uncontrolled hypertension had similar rates of short-term (at 3 and 6 months) and long-term (at 12 and 24 months) clinical outcomes. The two computable definitions generated consistent results.
Conclusions: Computable definitions can be successfully applied to health system EHR data to conduct population surveillance for hypertension and identify patients with uncontrolled hypertension who may benefit from additional treatment.
Keywords: Blood pressure; computable algorithm; electronic health records; hypertension.
Figures


References
-
- Adams JM and Wright JS. A National Commitment to Improve the Care of Patients With Hypertension in the US. JAMA. 2020. - PubMed
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr., Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr., Williamson JD and Wright JT Jr. 2017. ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2018;138:e426–e483. - PubMed
-
- Jollis JG, Ancukiewicz M, DeLong ER, Pryor DB, Muhlbaier LH and Mark DB. Discordance of databases designed for claims payment versus clinical information systems. Implications for outcomes research. Ann Intern Med. 1993;119:844–50. - PubMed
-
- Hartzema AG, Racoosin JA, MaCurdy TE, Gibbs JM and Kelman JA. Utilizing Medicare claims data for real-time drug safety evaluations:is it feasible? Pharmacoepidemiol Drug Saf. 2011;20:684–8. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources