

This is a preprint.
Time-to-Event Genome-Wide Association Study for Incident Cardiovascular Disease in People with Type 2 Diabetes Mellitus
- PMID: 37546893
- PMCID: PMC10402212
- DOI: 10.1101/2023.07.25.23293180
Time-to-Event Genome-Wide Association Study for Incident Cardiovascular Disease in People with Type 2 Diabetes Mellitus
Update in
-
Time-to-Event Genome-Wide Association Study for Incident Cardiovascular Disease in People With Type 2 Diabetes.Diabetes Care. 2024 Jun 1;47(6):1042-1047. doi: 10.2337/dc23-2274. Diabetes Care. 2024. PMID: 38652672 Free PMC article.
Abstract
Background: Type 2 diabetes mellitus (T2D) confers a two- to three-fold increased risk of cardiovascular disease (CVD). However, the mechanisms underlying increased CVD risk among people with T2D are only partially understood. We hypothesized that a genetic association study among people with T2D at risk for developing incident cardiovascular complications could provide insights into molecular genetic aspects underlying CVD.
Methods: From 16 studies of the Cohorts for Heart & Aging Research in Genomic Epidemiology (CHARGE) Consortium, we conducted a multi-ancestry time-to-event genome-wide association study (GWAS) for incident CVD among people with T2D using Cox proportional hazards models. Incident CVD was defined based on a composite of coronary artery disease (CAD), stroke, and cardiovascular death that occurred at least one year after the diagnosis of T2D. Cohort-level estimated effect sizes were combined using inverse variance weighted fixed effects meta-analysis. We also tested 204 known CAD variants for association with incident CVD among patients with T2D.
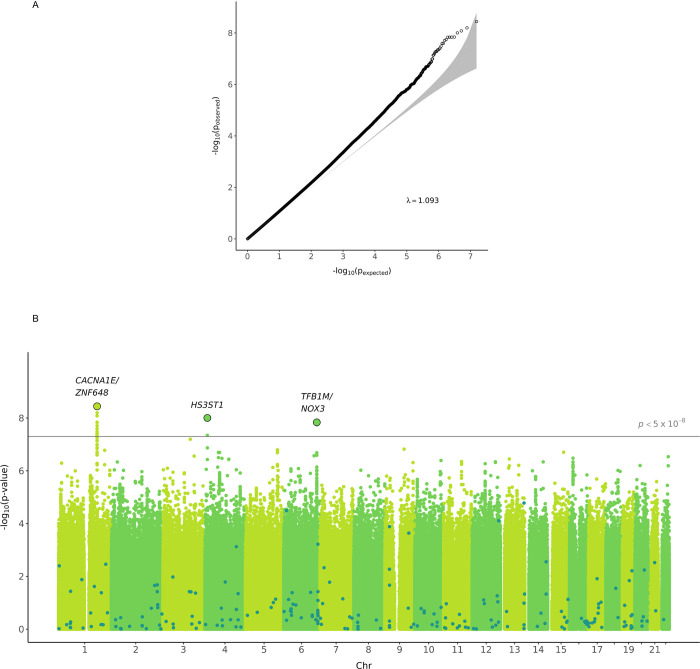
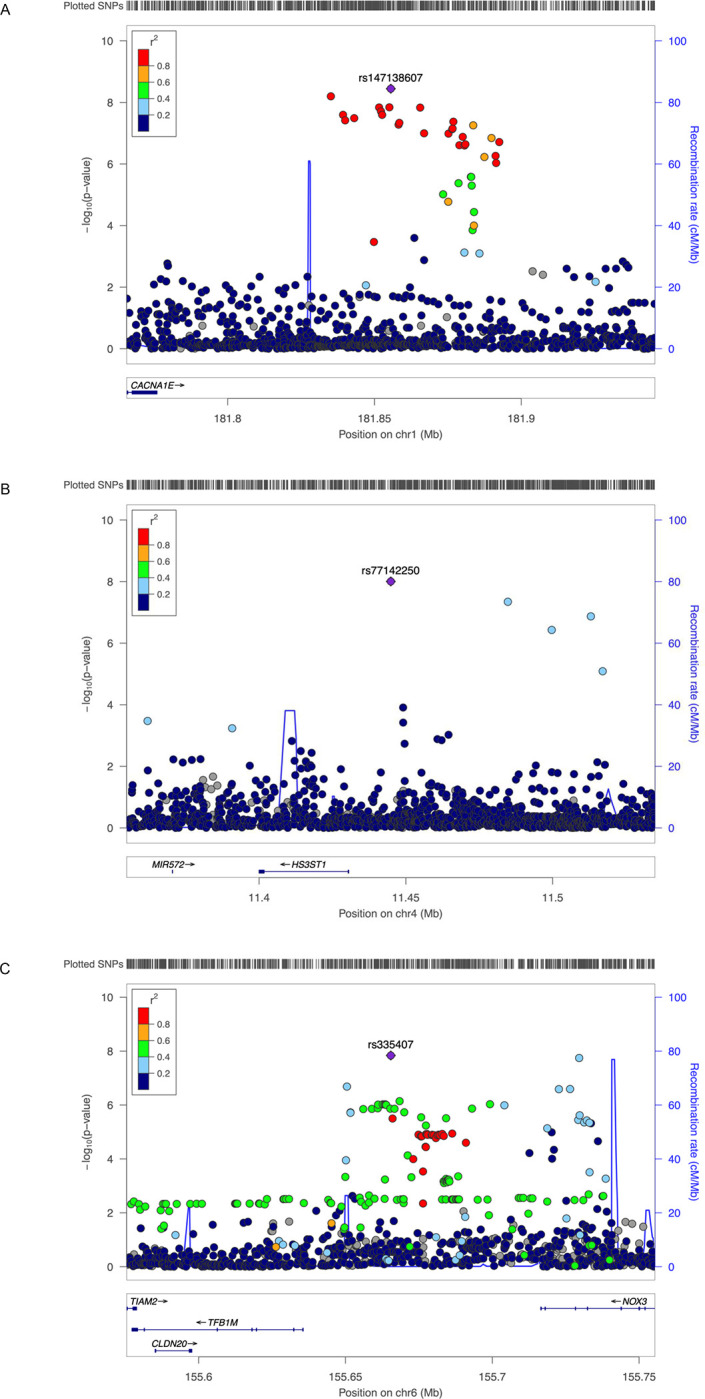
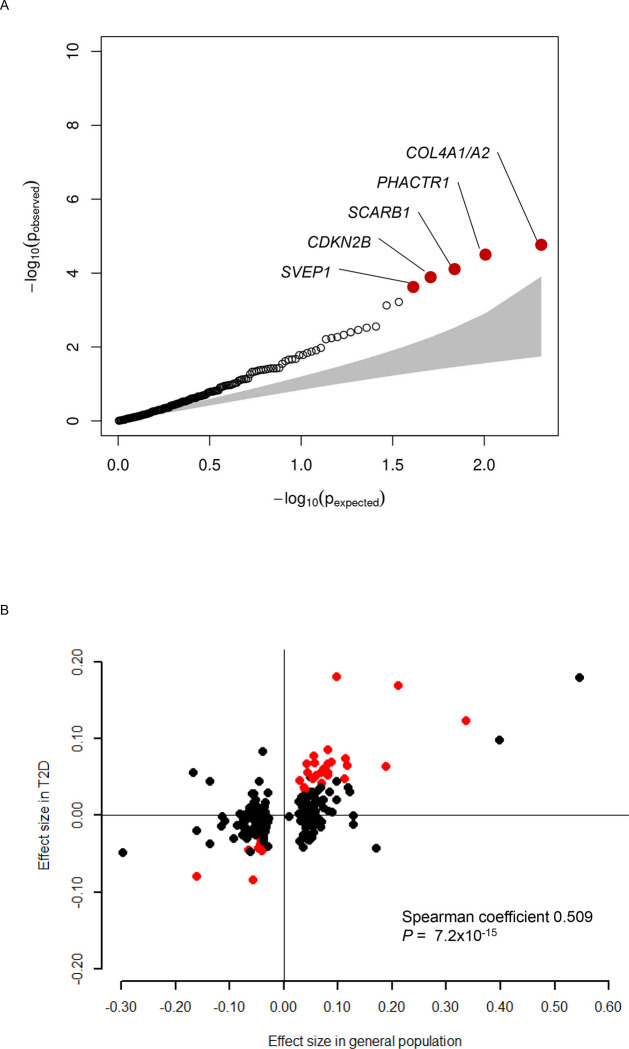
Results: A total of 49,230 participants with T2D were included in the analyses (31,118 European ancestries and 18,112 non-European ancestries) which consisted of 8,956 incident CVD cases over a range of mean follow-up duration between 3.2 and 33.7 years (event rate 18.2%). We identified three novel, distinct genetic loci for incident CVD among individuals with T2D that reached the threshold for genome-wide significance (P<5.0×10-8): rs147138607 (intergenic variant between CACNA1E and ZNF648) with a hazard ratio (HR) 1.23, 95% confidence interval (CI) 1.15 - 1.32, P=3.6×10-9, rs11444867 (intergenic variant near HS3ST1) with HR 1.89, 95% CI 1.52 - 2.35, P=9.9×10-9, and rs335407 (intergenic variant between TFB1M and NOX3) HR 1.25, 95% CI 1.16 - 1.35, P=1.5×10-8. Among 204 known CAD loci, 32 were associated with incident CVD in people with T2D with P<0.05, and 5 were significant after Bonferroni correction (P<0.00024, 0.05/204). A polygenic score of these 204 variants was significantly associated with incident CVD with HR 1.14 (95% CI 1.12 - 1.16) per 1 standard deviation increase (P=1.0×10-16).
Conclusions: The data point to novel and known genomic regions associated with incident CVD among individuals with T2D.
Figures
References
-
- Haffner SM, Lehto S, Ronnemaa T, Pyorala K and Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339:229–34. - PubMed
-
- Kannel WB and McGee DL. Diabetes and cardiovascular disease. The Framingham study. JAMA. 1979;241:2035–8. - PubMed
-
- Rosenquist KJ and Fox CS. Mortality Trends in Type 2 Diabetes. In: rd, Cowie C. C., Casagrande S. S, Menke A, Cissell M. A, Eberhardt M. S, Meigs J. B, Gregg E. W, Knowler W. C, Barrett-Connor E, Becker D. J., Brancati F. L, Boyko E. J, Herman W. H, Howard B. V, Narayan K. M. V, Rewers Mand Fradkin J. E, eds. Diabetes in America Bethesda (MD); 2018. - PubMed
-
- Rawshani A, Rawshani A, Franzen S, Eliasson B, Svensson AM, Miftaraj M, McGuire DK, Sattar N, Rosengren A and Gudbjornsdottir S. Mortality and Cardiovascular Disease in Type 1 and Type 2 Diabetes. N Engl J Med. 2017;376:1407–1418. - PubMed
-
- Goff DC Jr., Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R, Greenland P, Lackland DT, Levy D, O’Donnell CJ, Robinson JG, Schwartz JS, Shero ST, Smith SC Jr., Sorlie P, Stone NJ, Wilson PW, Jordan HS, Nevo L, Wnek J, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Smith SC Jr, Tomaselli GF and American College of Cardiology/American Heart Association Task Force on Practice G. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S49–73. - PubMed
Publication types
Grants and funding
- 75N92021D00005/WH/WHI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- R01 HL162928/HL/NHLBI NIH HHS/United States
- R01 HL159514/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- HHSN268201800015I/HB/NHLBI NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- N01 HC085080/HL/NHLBI NIH HHS/United States
- R01 HL103612/HL/NHLBI NIH HHS/United States
- 75N92020D00002/HL/NHLBI NIH HHS/United States
- 75N92021D00002/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- HHSN268201800012I/HB/NHLBI NIH HHS/United States
- HHSN268201800012C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- 75N92020D00005/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- R01 HL120393/HL/NHLBI NIH HHS/United States
- HHSN268201500001C/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N02 HL064278/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- UL1 TR001878/TR/NCATS NIH HHS/United States
- HHSN268201800014I/HB/NHLBI NIH HHS/United States
- R01 HL043851/HL/NHLBI NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- R01 HL085251/HL/NHLBI NIH HHS/United States
- 75N92020D00001/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- S10 OD028685/OD/NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- R01 HL087652/HL/NHLBI NIH HHS/United States
- T32 HL007457/HL/NHLBI NIH HHS/United States
- HHSN268201800014C/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01 HL136666/HL/NHLBI NIH HHS/United States
- 75N92020D00003/HL/NHLBI NIH HHS/United States
- R01 HL105756/HL/NHLBI NIH HHS/United States
- 75N92021D00001/HL/NHLBI NIH HHS/United States
- P30 DK063491/DK/NIDDK NIH HHS/United States
- R01 DK109588/DK/NIDDK NIH HHS/United States
- R01 HL146860/HL/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- HHSN268201800013I/MD/NIMHD NIH HHS/United States
- IK2 CX001780/CX/CSRD VA/United States
- U01 NS041588/NS/NINDS NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- 75N92021D00003/WH/WHI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- U01 HG011723/HG/NHGRI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- 75N92020D00004/HL/NHLBI NIH HHS/United States
- UM1 CA182913/CA/NCI NIH HHS/United States
- 75N92020D00007/HL/NHLBI NIH HHS/United States
- T32 GM100842/GM/NIGMS NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- HHSN268201800011C/HL/NHLBI NIH HHS/United States
- R01 CA047988/CA/NCI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- 75N92021D00006/HL/NHLBI NIH HHS/United States
- R01 HL080467/HL/NHLBI NIH HHS/United States
- 75N92019D00031/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- R01 HL151855/HL/NHLBI NIH HHS/United States
- HHSN268201800010I/HB/NHLBI NIH HHS/United States
- UM1 DK078616/DK/NIDDK NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- 75N92020D00006/HL/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- HHSN268201800011I/HB/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- R01 HL142809/HL/NHLBI NIH HHS/United States
- 75N92021D00004/WH/WHI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Miscellaneous