

Transvalvular Unloading Mitigates Ventricular Injury Due to Venoarterial Extracorporeal Membrane Oxygenation in Acute Myocardial Infarction
- PMID: 37547066
- PMCID: PMC10401286
- DOI: 10.1016/j.jacbts.2023.01.004
Transvalvular Unloading Mitigates Ventricular Injury Due to Venoarterial Extracorporeal Membrane Oxygenation in Acute Myocardial Infarction
Abstract
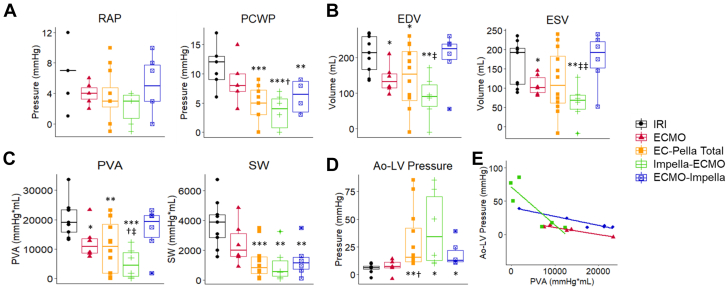
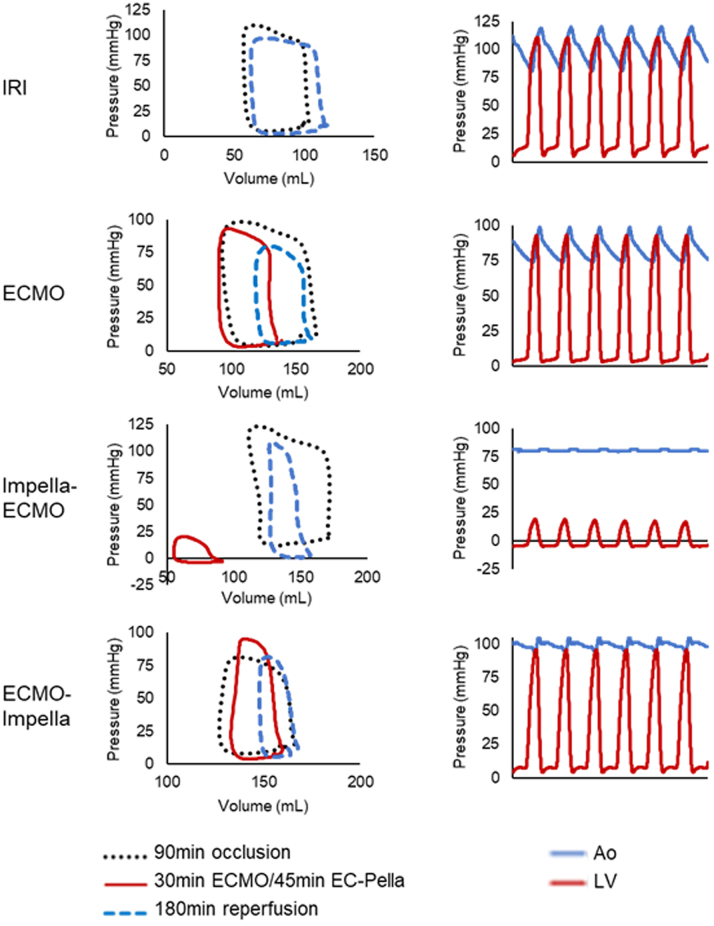
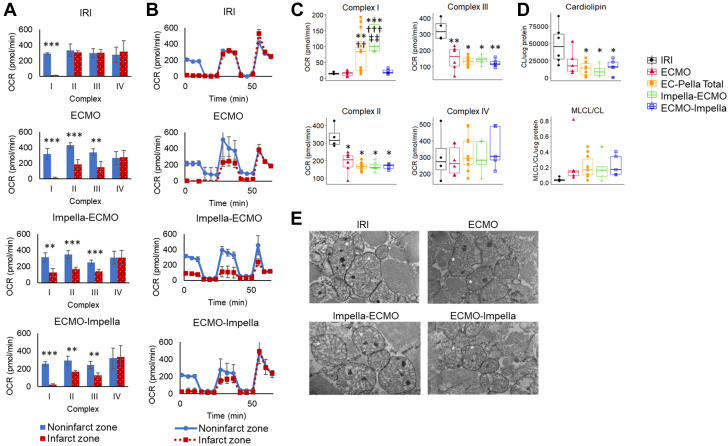
Whether extracorporeal membrane oxygenation (ECMO) with Impella, known as EC-Pella, limits cardiac damage in acute myocardial infarction remains unknown. The authors now report that the combination of transvalvular unloading and ECMO (EC-Pella) initiated before reperfusion reduced infarct size compared with ECMO alone before reperfusion in a preclinical model of acute myocardial infarction. EC-Pella also reduced left ventricular pressure-volume area when transvalvular unloading was applied before, not after, activation of ECMO. The authors further observed that EC-Pella increased cardioprotective signaling but failed to rescue mitochondrial dysfunction compared with ECMO alone. These findings suggest that ECMO can increase infarct size in acute myocardial infarction and that EC-Pella can mitigate this effect but also suggest that left ventricular unloading and myocardial salvage may be uncoupled in the presence of ECMO in acute myocardial infarction. These observations implicate mechanisms beyond hemodynamic load as part of the injury cascade associated with ECMO in acute myocardial infarction.
Keywords: cardioprotection; hemodynamic status; mechanical circulatory support; unloading.
© 2023 The Authors.
Conflict of interest statement
This work was supported by National Institutes of Health grants R01HL159089-01 and R01HL139785-01. Dr Kapur has received consulting and speaker honoraria and institutional grant support from Abbott Laboratories, Abiomed, Boston Scientific, Edwards Lifesciences, LivaNova, Getinge, and Zoll. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



References
-
- Fried J.A., Griffin J.M., Masoumi A., et al. Predictors of survival and ventricular recovery following acute myocardial infarction requiring extracorporeal membrane oxygenation therapy. ASAIO J. 2022;68(6):800–807. - PubMed
-
- Sheu J.J., Tsai T.H., Lee F.Y., et al. Early extracorporeal membrane oxygenator-assisted primary percutaneous coronary intervention improved 30-day clinical outcomes in patients with ST-segment elevation myocardial infarction complicated with profound cardiogenic shock. Crit Care Med. 2010;38(9):1810–1817. - PubMed
LinkOut - more resources
Full Text Sources
