

Long-Term Efficacy and Safety of Rituximab Versus Tacrolimus in Children With Steroid Dependent Nephrotic Syndrome
- PMID: 37547526
- PMCID: PMC10403658
- DOI: 10.1016/j.ekir.2023.05.022
Long-Term Efficacy and Safety of Rituximab Versus Tacrolimus in Children With Steroid Dependent Nephrotic Syndrome
Abstract
Introduction: In the Rituximab for Relapse Prevention in Nephrotic Syndrome (RITURNS) trial, we demonstrated superior efficacy of single-course rituximab over maintenance tacrolimus in preventing relapses in children with steroid dependent nephrotic syndrome (SDNS) during a 1-year observation. Here we present the long-term outcomes of all 117 trial completers, who were followed up for another 2 years.
Methods: Relapsing patients in the rituximab arm received a second course of rituximab, either with (n = 44) or without mycophenolate mofetil (MMF) cotreatment (n = 15). In the tacrolimus arm, second line rituximab monotherapy was initiated after relapses (n = 32) or electively (n = 24).
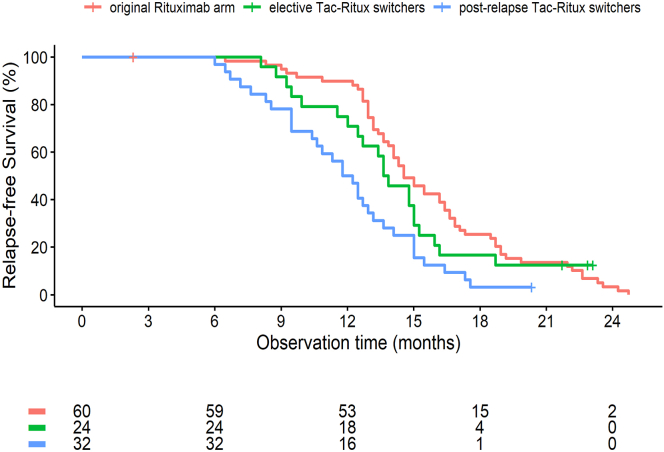
Results: All 12-month relapse-free patients in the rituximab arm relapsed in the second postexposure year, resulting in similar median relapse-free survival times in the 2 trial arms (62 vs. 59 weeks). Second line rituximab in the tacrolimus arm was less effective than first-line therapy in patients switched to rituximab following a relapse (relapse-free survival 55 vs. 63 weeks, P < 0.01). B-cell counts 6 months post-rituximab predicted relapse risk both for first and second line therapy. MMF cotreatment yielded much improved 2-year relapse-free survival as compared to rituximab monotherapy (67% vs. 9%, P < 0.0001). Higher grade 2 adverse event rates were observed post-rituximab versus on tacrolimus (0.87 vs. 0.53 per year).
Conclusion: The superior therapeutic effect of rituximab in SDNS vanishes during the second year post-exposure. Rituximab appears to yield longer remission when applied as first line as compared to second line therapy. Maintenance MMF following rituximab induces long-term disease remission.
Keywords: childhood nephrotic syndrome; rituximab; steroid dependent nephrotic syndrome; tacrolimus.
© 2023 International Society of Nephrology. Published by Elsevier Inc.
Figures




Comment in
-
Children with Steroid Dependent Nephrotic Syndrome: Rituximab or Tacrolimus? It's All in the Timing.Kidney Int Rep. 2023 Aug 6;8(9):1708-1710. doi: 10.1016/j.ekir.2023.07.016. eCollection 2023 Sep. Kidney Int Rep. 2023. PMID: 37705906 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
