

Comparing the Effect of Implanted Peroneal Nerve Stimulation and Ankle-Foot Orthosis on Gait Kinematics in Chronic Hemiparesis: A Randomized Controlled Trial
- PMID: 37548420
- PMCID: PMC10424098
- DOI: 10.2340/jrm.v55.7130
Comparing the Effect of Implanted Peroneal Nerve Stimulation and Ankle-Foot Orthosis on Gait Kinematics in Chronic Hemiparesis: A Randomized Controlled Trial
Abstract
Objective: Impaired ankle dorsiflexion in hemiparesis may be treated with ankle-foot orthosis or functional electrical stimulation. Semi-implanted selective functional electrical stimulation uses independent stimulations of deep and superficial peroneal nerves. The aim of this study was to compare gait kinematics using ankle-foot orthosis or semi-implanted selective functional electrical stimulation over 6 months in hemiparesis.
Methods: Subjects with chronic hemiparesis, randomized into ankle-foot orthosis or semi-implanted selective functional electrical stimulation groups, underwent comfortable gait analysis without and with device OFF and ON, before, and 3 and 6 months after treatment onset. The effects of condition, visit and group on gait kinematics (analysis of variance; ANOVA) were analysed.
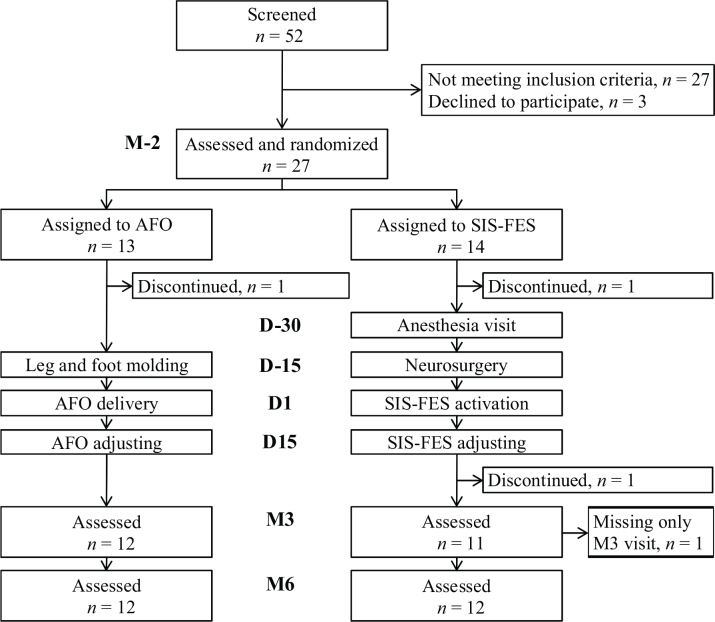
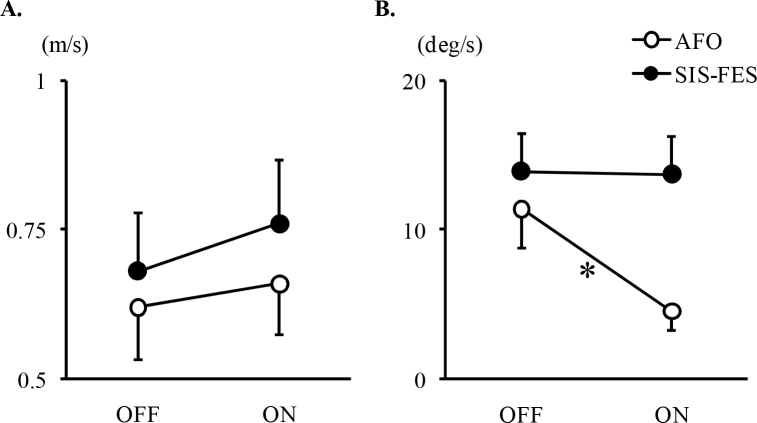
Results: A total of 27 subjects were included (ankle-foot orthosis, n = 13; semi-implanted selective functional electrical stimulation, n = 14). The only between-group difference in changes from OFF to ON conditions was a deteriorated ankle dorsiflexion speed with ankle-foot orthosis at month 6 (condition*group, p = 0.04; ankle-foot orthosis, -60%, p = 0.02; semi-implanted selective functional electrical stimulation, non significant). Both groups pooled, from OFF to ON gait speed (+ 0.07 m/s; + 10%), cadence (+ 4%), step length (+ 6%) and peak ankle dorsiflexion (+ 6°) increased, and peak ankle inversion (-5°) and peak knee flexion (-2°) decreased (p < 0.001); finally, peak knee flexion in the OFF condition increased (+ 2°, p = 0.03).
Conclusion: Semi-implanted selective functional electrical stimulation and ankle-foot orthosis similarly impacted gait kinematics in chronic hemiparesis after 6 months of use. Ankle dorsiflexion speed in swing deteriorated markedly with ankle-foot orthosis.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
