

Exploring Hikikomori-like idiom of distress a year into the SARS-CoV-2 pandemic in Oman: Factorial validity of the 25-item Hikikomori Questionnaire, prevalence and associated factors
- PMID: 37549148
- PMCID: PMC10406187
- DOI: 10.1371/journal.pone.0279612
Exploring Hikikomori-like idiom of distress a year into the SARS-CoV-2 pandemic in Oman: Factorial validity of the 25-item Hikikomori Questionnaire, prevalence and associated factors
Abstract
Background: Existing literature that examines the Hikikomori-like idiom of distress (HLID) initially labelled this phenomenon as a culture-bound syndrome. However, the increasing number of reports from other parts of the world suggest that HLID could instead be a culture-reactive idiom of distress, originating from biopsychosocial disequilibrium and cultural upheaval. The impact of imposed social withdrawal due to the Coronavirus 2 severe acute respiratory syndrome (SARS-CoV-2) pandemic on the growing prevalence of HLID has not yet been adequately explored. Aims: The first objective is to examine the factorial validity of the 25-item Hikikomori Questionnaire (HQ-25) in Oman. Second, we aimed to investigate the prevalence of HLID following the lifting of SARS-COV-2 restrictions in the Arabian Gulf country of Oman. The third related objective is to examine factors associated with the variation of HLID.
Methods: This cross-sectional online survey was widely distributed across the diverse socio-demographic population residing in Oman. After the validation of the questionnaire and the factorial validity, the Arabic version of HQ-25 was used to explore the prevalence and factors associated with HLID.
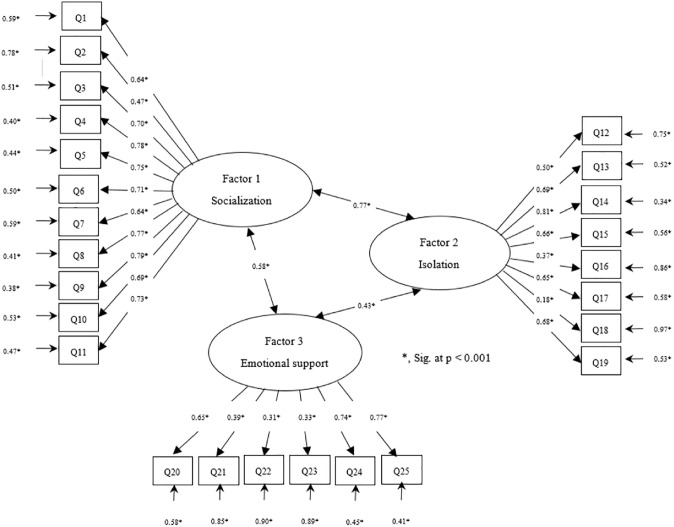
Results: A total of 1529 participants were included in the study (response rate = 76.5%), of whom 44% (n = 673) expressed HLID. We randomly split it into half, one for exploratory factor analysis (EFA) (n = 764) and the other half for confirmatory factor analysis (CFA) (n = 765). From the EFA results, a three-factor model was found for the Omani version of HQ-25, which represented 52.87% of the variance with good internal reliability (Overall Cronbach's: 0.92; Socialisation: 0.92; Isolation: 0.84; Emotional support: 0.73). The CFA results report acceptable goodness-of-fit indices (χ2/df = 17.92, p < .001; CFI = 0.90; TLI = 0.95; RMSEA = 0.04, 95% CI 0.02-0.07; SRMR = 0.05) of the three-factor model of the collected samples. All 1529 data were used in the respondents. The results of the logistic regression showed that married marital status (OR = 1.51, 95% CI: 1.12-2.03, p = 0.007), older age (OR = 0.97, 95% CI: 0.95-0.99, p = 0.008), living in an urban area (OR = 0.71, 95% CI: 0.56-0.91, p = 0.006), unemployed occupational status (OR = 1.72, 95% CI: 1.30-2.88, p < .001), screen time (7+ hours vs. <4 hours: OR = 4.50, 95% CI: 3.16-6.41, p < .001; 4-7 hours vs. <4 hours: OR = 2.10, 95% CI: 1.61-2.70, p < .001), history of mental illness (OR = 3.70, 95% CI: 2.29-5.91, p < .001), and adverse childhood experiences (OR = 2.60, 95% CI: 2.03-3.20, p < .001) were significant risk factors for HLID.
Conclusion: The factorial validity of the HQ-25 performed in this study appears to mirror the previously reported 3-factor structures. Some of the associated factors appear to support and, conversely, dissent from the findings of previous studies. These are discussed in terms of the attributions of the SARS-COV-2 pandemic, demographic trends in Oman, and sociocultural factors specific to the region of interest.
Copyright: © 2023 Al-Sibani et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Norasakkunkit V, Uchida Y. To conform or to maintain self-consistency? Hikikomori risk in Japan and the deviation from seeking harmony. J Soc Clin Psychol. 2014;33: 918.
-
- Tajan N. Social withdrawal and psychiatry: A comprehensive review of Hikikomori. Neuropsychiatrie de l’Enfance et de l’Adolescence. 2015;63: 324–331.
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
