

Estimating Breast Cancer Overdiagnosis After Screening Mammography Among Older Women in the United States
- PMID: 37549389
- PMCID: PMC10623662
- DOI: 10.7326/M23-0133
Estimating Breast Cancer Overdiagnosis After Screening Mammography Among Older Women in the United States
Abstract
Background: Overdiagnosis is increasingly recognized as a harm of breast cancer screening, particularly for older women.
Objective: To estimate overdiagnosis associated with breast cancer screening among older women by age.
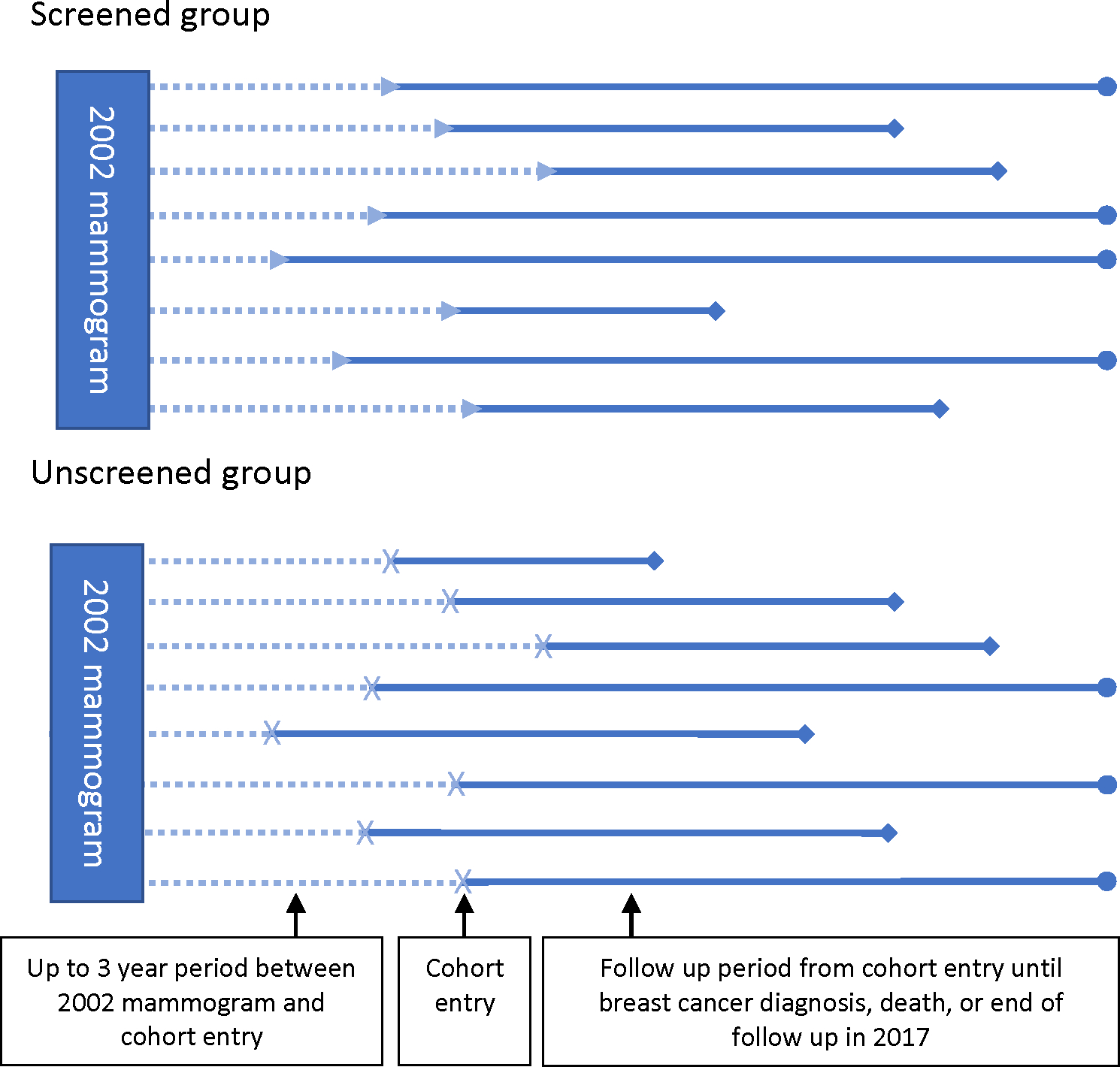
Design: Retrospective cohort study comparing the cumulative incidence of breast cancer among older women who continued screening in the next interval with those who did not. Analyses used competing risk models, stratified by age.
Setting: Fee-for-service Medicare claims, linked to the SEER (Surveillance, Epidemiology, and End Results) program.
Patients: Women 70 years and older who had been recently screened.
Measurements: Breast cancer diagnoses and breast cancer death for up to 15 years of follow-up.
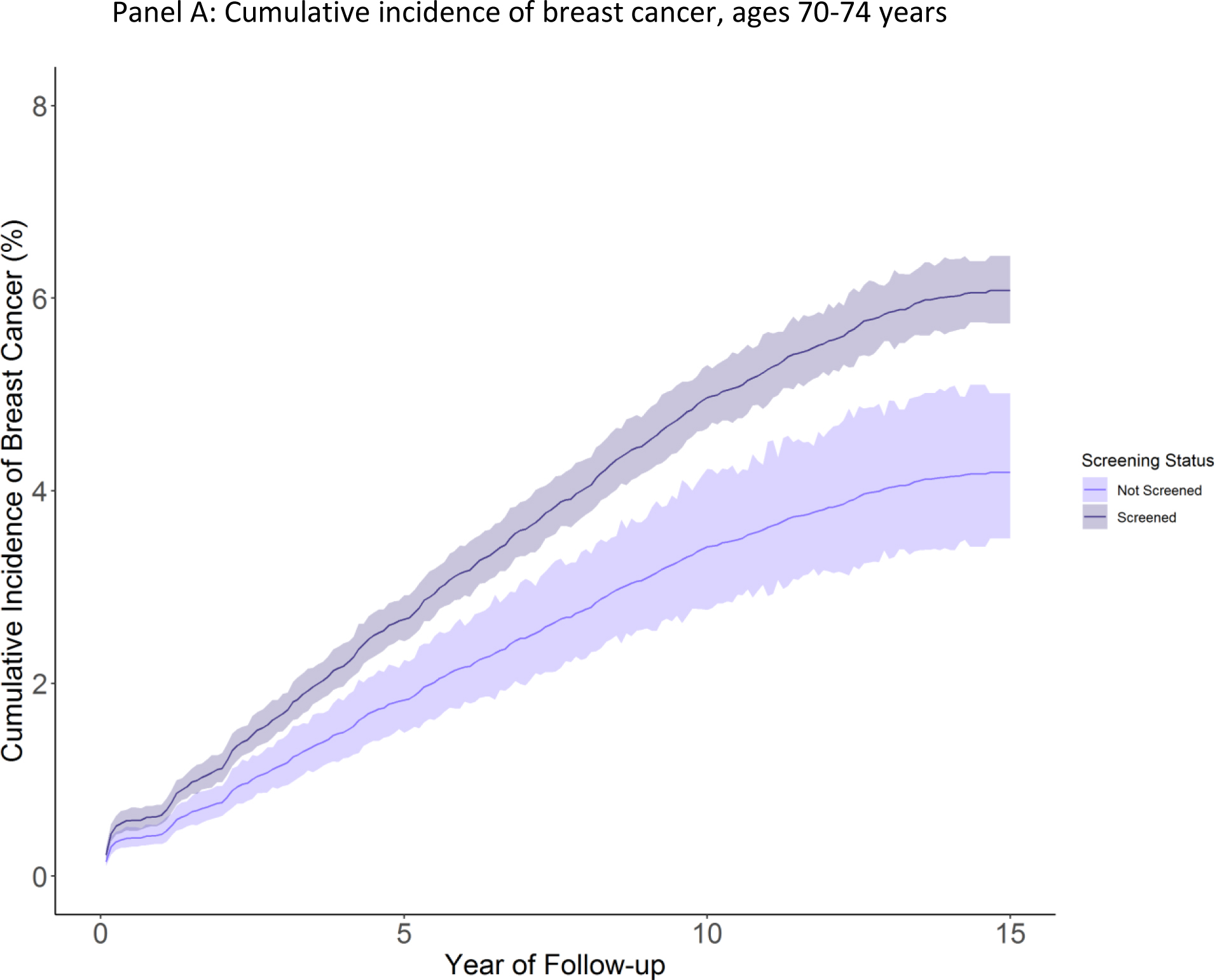
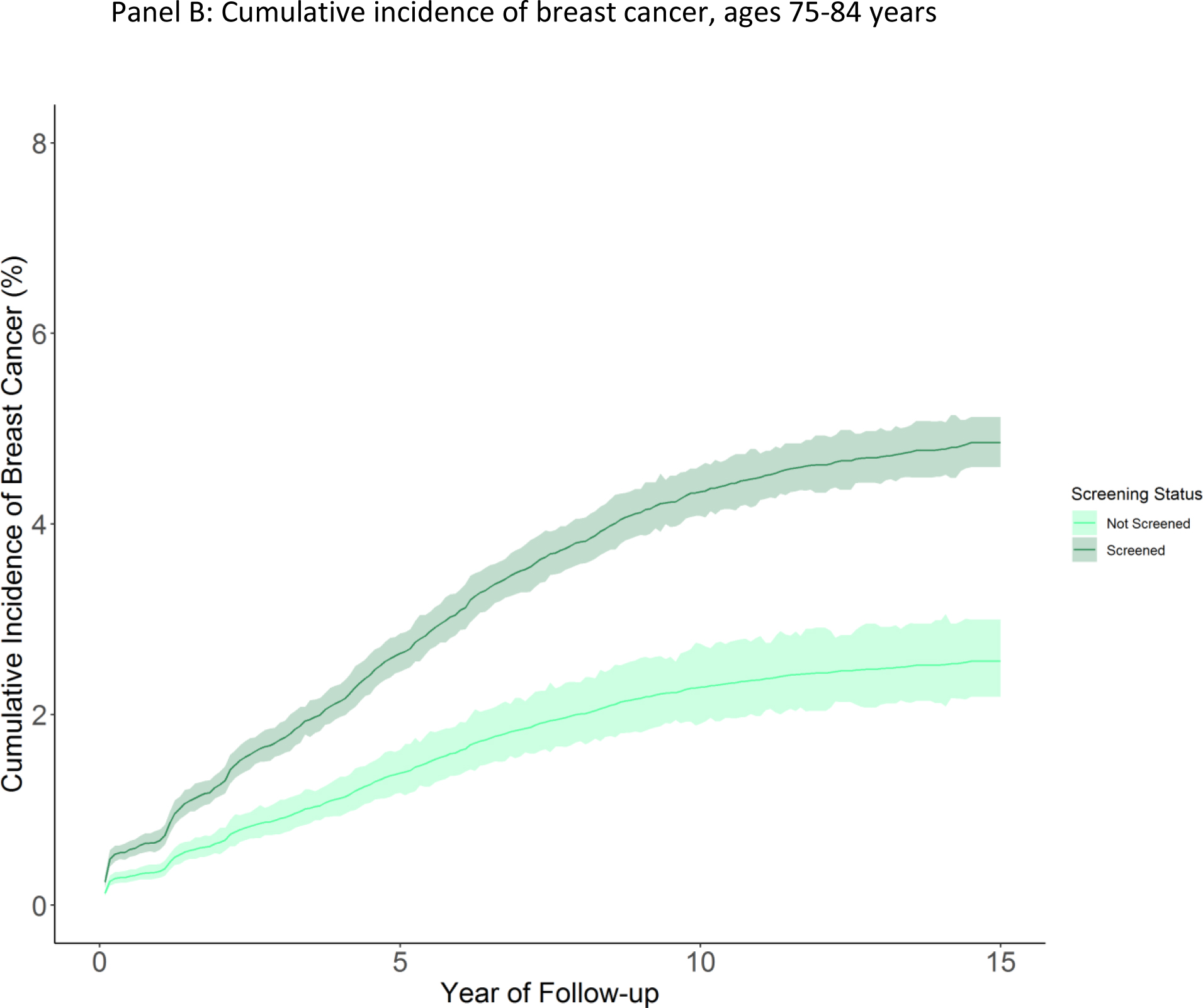
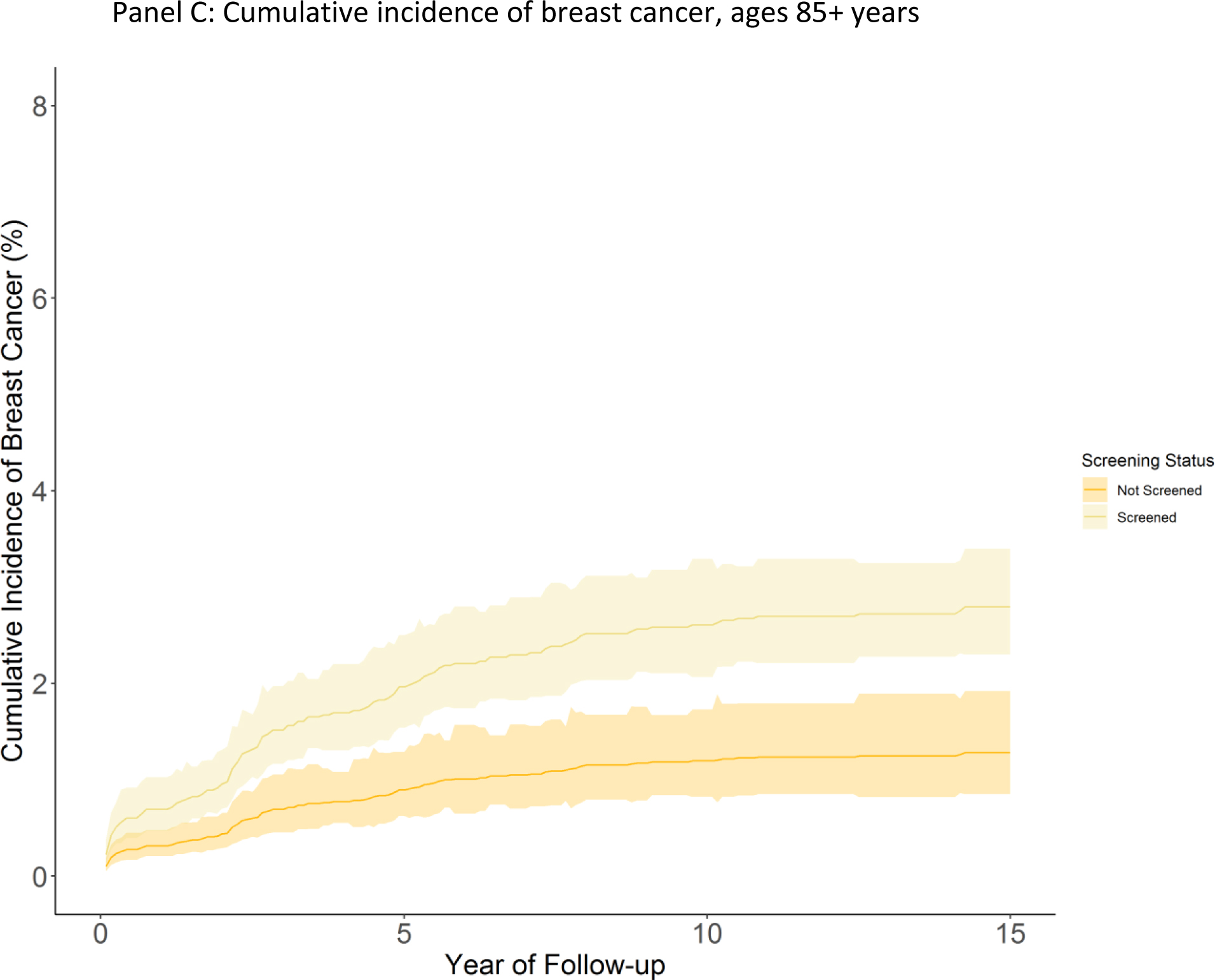
Results: This study included 54 635 women. Among women aged 70 to 74 years, the adjusted cumulative incidence of breast cancer was 6.1 cases (95% CI, 5.7 to 6.4) per 100 screened women versus 4.2 cases (CI, 3.5 to 5.0) per 100 unscreened women. An estimated 31% of breast cancer among screened women were potentially overdiagnosed. For women aged 75 to 84 years, cumulative incidence was 4.9 (CI, 4.6 to 5.2) per 100 screened women versus 2.6 (CI, 2.2 to 3.0) per 100 unscreened women, with 47% of cases potentially overdiagnosed. For women aged 85 and older, the cumulative incidence was 2.8 (CI, 2.3 to 3.4) among screened women versus 1.3 (CI, 0.9 to 1.9) among those not, with up to 54% overdiagnosis. We did not see statistically significant reductions in breast cancer-specific death associated with screening.
Limitations: This study was designed to estimate overdiagnosis, limiting our ability to draw conclusions on all benefits and harms of screening. Unmeasured differences in risk for breast cancer and differential competing mortality between screened and unscreened women may confound results. Results were sensitive to model specifications and definition of a screening mammogram.
Conclusion: Continued breast cancer screening was associated with greater incidence of breast cancer, suggesting overdiagnosis may be common among older women who are diagnosed with breast cancer after screening. Whether harms of overdiagnosis are balanced by benefits and for whom remains an important question.
Primary funding source: National Cancer Institute.
Conflict of interest statement
Figures
Comment in
-
Understanding the Varying Biological Behaviors of Breast and Other Types of Cancer to Avoid Overdiagnosis.Ann Intern Med. 2023 Sep;176(9):1273-1274. doi: 10.7326/M23-1895. Epub 2023 Aug 8. Ann Intern Med. 2023. PMID: 37549388 No abstract available.
-
Estimating Breast Cancer Overdiagnosis After Screening Mammography Among Older Women in the United States.Ann Intern Med. 2024 Mar;177(3):403. doi: 10.7326/L23-0484. Ann Intern Med. 2024. PMID: 38498895 No abstract available.
References
-
- No Title. In: Health, United States, 2016: With Chartbook on Long-term Trends in Health [Internet]. Hyattsville (MD); 2017. Available from: https://www.ncbi.nlm.nih.gov/pubmed/28910066 - PubMed
-
- Walter LC, Schonberg MA. Screening mammography in older women: a review. JAMA [Internet]. 2014;311(13):1336–47. Available from: https://www.ncbi.nlm.nih.gov/pubmed/24691609 - PMC - PubMed
-
- Nelson HD, Cantor A, Humphrey L, Fu R, Pappas M, Daeges M, et al. Screening for Breast Cancer [Internet]. Screening for Breast Cancer: A Systematic Review to Update the 2009 U.S. Preventive Services Task Force Recommendation. Agency for Healthcare Research and Quality (US); 2016. [cited 2017 Feb 22]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26889531 - PubMed
-
- Lansdorp-Vogelaar I, Gulati R, Mariotto AB, Schechter CB, de Carvalho TM, Knudsen AB, et al. Personalizing age of cancer screening cessation based on comorbid conditions: model estimates of harms and benefits. Ann Intern Med [Internet]. 2014;161(2):104–12. Available from: https://www.ncbi.nlm.nih.gov/pubmed/25023249 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical