

Differences between patients in whom physicians agree versus disagree about the preoperative diagnosis of heart failure
- PMID: 37549434
- PMCID: PMC11221412
- DOI: 10.1016/j.jclinane.2023.111226
Differences between patients in whom physicians agree versus disagree about the preoperative diagnosis of heart failure
Abstract
Study objective: To quantify preoperative heart failure (HF) diagnostic agreement and identify characteristics of patients in whom physicians agreed versus disagreed about the diagnosis.
Design: Observational cohort study.
Setting: Patients undergoing major non-cardiac surgery at an academic center between 2015 and 2019.
Patients: 40,659 patients undergoing major non-cardiac surgery, among which a stratified subsample of 1018 patients with and without documented HF was reviewed.
Interventions: Via a panel of physicians frequently managing patients with HF (cardiologists, cardiac anesthesiologists, intensivists), detailed chart reviews were performed (two per patient; median review time 32 min per reviewer per patient) to render adjudicated HF diagnoses.
Measurements: Adjudicated diagnostic agreement measures (percent agreement, Krippendorf's alpha) and univariate comparisons (standardized differences) between patients in whom physicians agreed versus disagreed about the preoperative HF diagnosis.
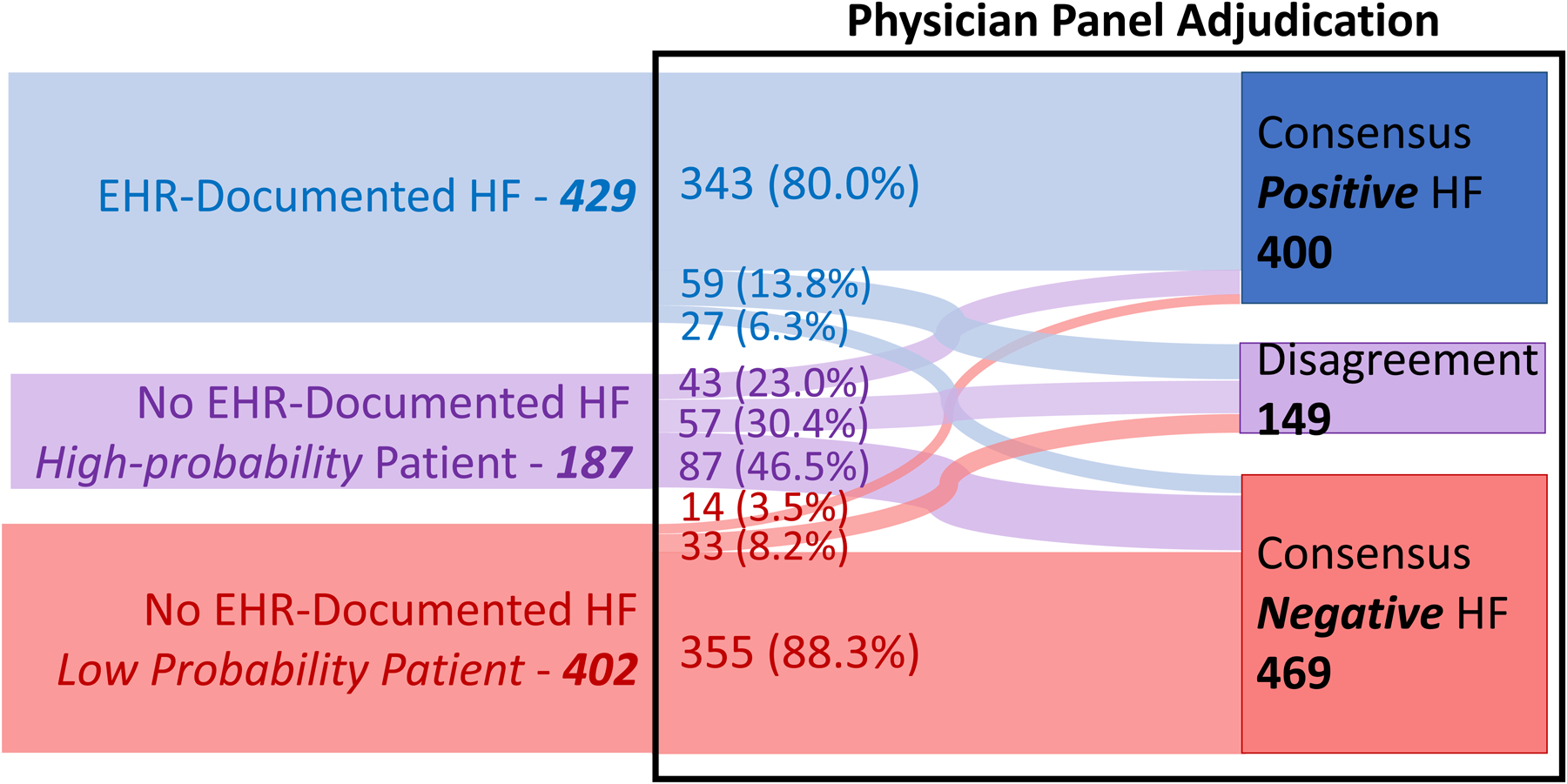
Main results: Among patients with documented HF, physicians agreed about the diagnosis in 80.0% of cases (consensus positive), disagreed in 13.8% (disagreement), and refuted the diagnosis in 6.3% (consensus negative). Conversely, among patients without documented HF, physicians agreed about the diagnosis in 88.0% (consensus negative), disagreed in 8.4% (disagreement), and refuted the diagnosis in 3.6% (consensus positive). The estimated agreement for the 40,659 cases was 91.1% (95% CI 88.3%-93.9%); Krippendorff's alpha was 0.77 (0.75-0.80). Compared to patients in whom physicians agreed about a HF diagnosis, patients in whom physicians disagreed exhibited fewer guideline-defined HF diagnostic criteria.
Conclusions: Physicians usually agree about HF diagnoses adjudicated via chart review, although disagreement is not uncommon and may be partly explained by heterogeneous clinical presentations. Our findings inform preoperative screening processes by identifying patients whose characteristics contribute to physician disagreement via chart review. Clinical Trial Number / Registry URL: Not applicable.
Keywords: Cardiac risk assessment; Diagnostic agreement; Electronic health record; Heart failure; Non-cardiac surgery; Preoperative evaluation.
Copyright © 2023. Published by Elsevier Inc.
Conflict of interest statement
Declaration of Competing Interest The authors declare: Dr. Mathis receives funding from the US National Institutes of Health (R01DK133226) unrelated to the present work. Dr. Golbus receives funding from the US National Institutes of Health (L30HL143700, 1K23HL168220–01) and National Science Foundation (Grant No. 2014003) and receives salary support by an American Heart Association grant (grant number 20SFRN35370008). Dr. Engoren serves on a data safety monitoring board for use of extracorporeal membrane oxygenation in patients with out-of-hospital cardiac arrest and for use of varying oxygenation strategies for patients with respiratory failure, unrelated to this work. Dr. Sjoding receives funding from the US National Institutes of Health (R01HL158626 and R01LM013325) unrelated to the present work. No other relationships or activities existed that could appear to have influenced the submitted work.
Figures



References
-
- Murphy SP, Ibrahim NE, Januzzi JL Jr. Heart Failure With Reduced Ejection Fraction: A Review. JAMA 2020;324:488–504. - PubMed
-
- Heart Association Council on Epidemiology A. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation 2020. - PubMed
-
- Duceppe E, Patel A, Chan MTV, Berwanger O, Ackland G, Kavsak PA, et al. Preoperative N-terminal pro-B-type natriuretic peptide and cardiovascular events after noncardiac surgery: A cohort study. Ann Intern Med 2020;172:96–104. - PubMed
-
- Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol 2014;64:e77–137. - PubMed
-
- Hammill BG, Curtis LH, Bennett-Guerrero E, O’Connor CM, Jollis JG, Schulman KA, et al. Impact of heart failure on patients undergoing major noncardiac surgery. Anesthesiology 2008;108:559–67. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
