

Gender-based research underscores sex differences in biological processes, clinical disorders and pharmacological interventions
- PMID: 37549793
- PMCID: PMC10587961
- DOI: 10.1016/j.bcp.2023.115737
Gender-based research underscores sex differences in biological processes, clinical disorders and pharmacological interventions
Abstract
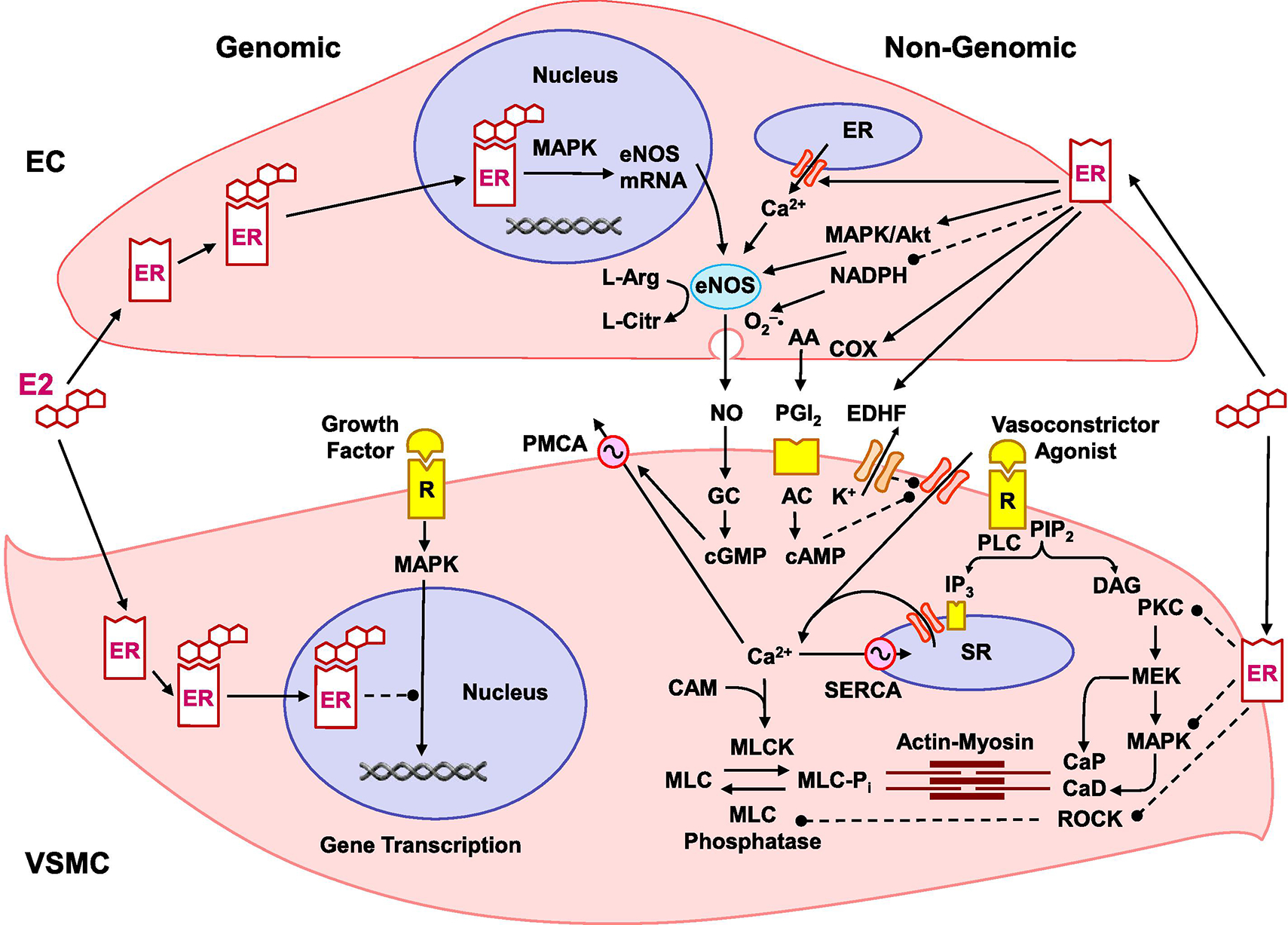
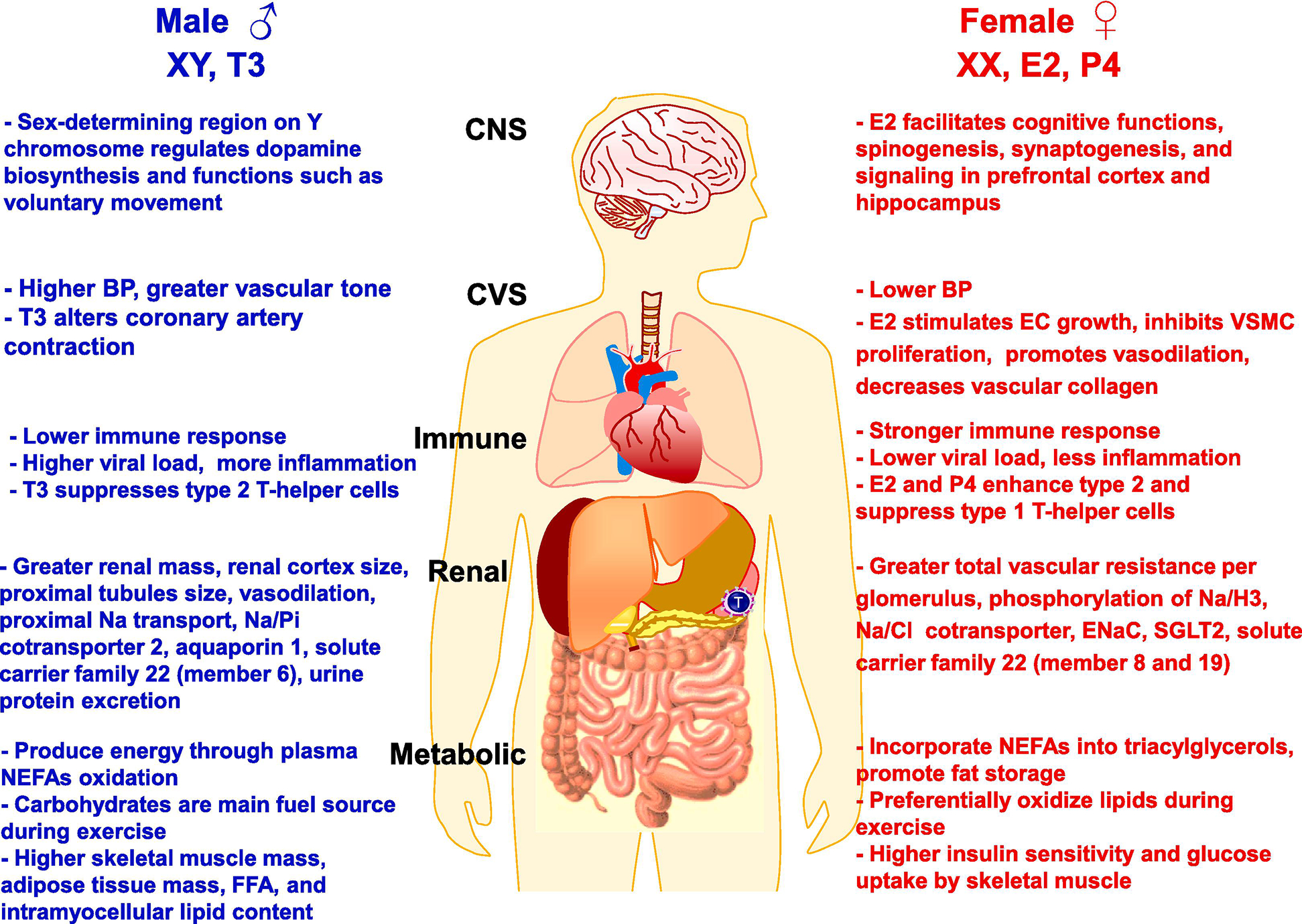
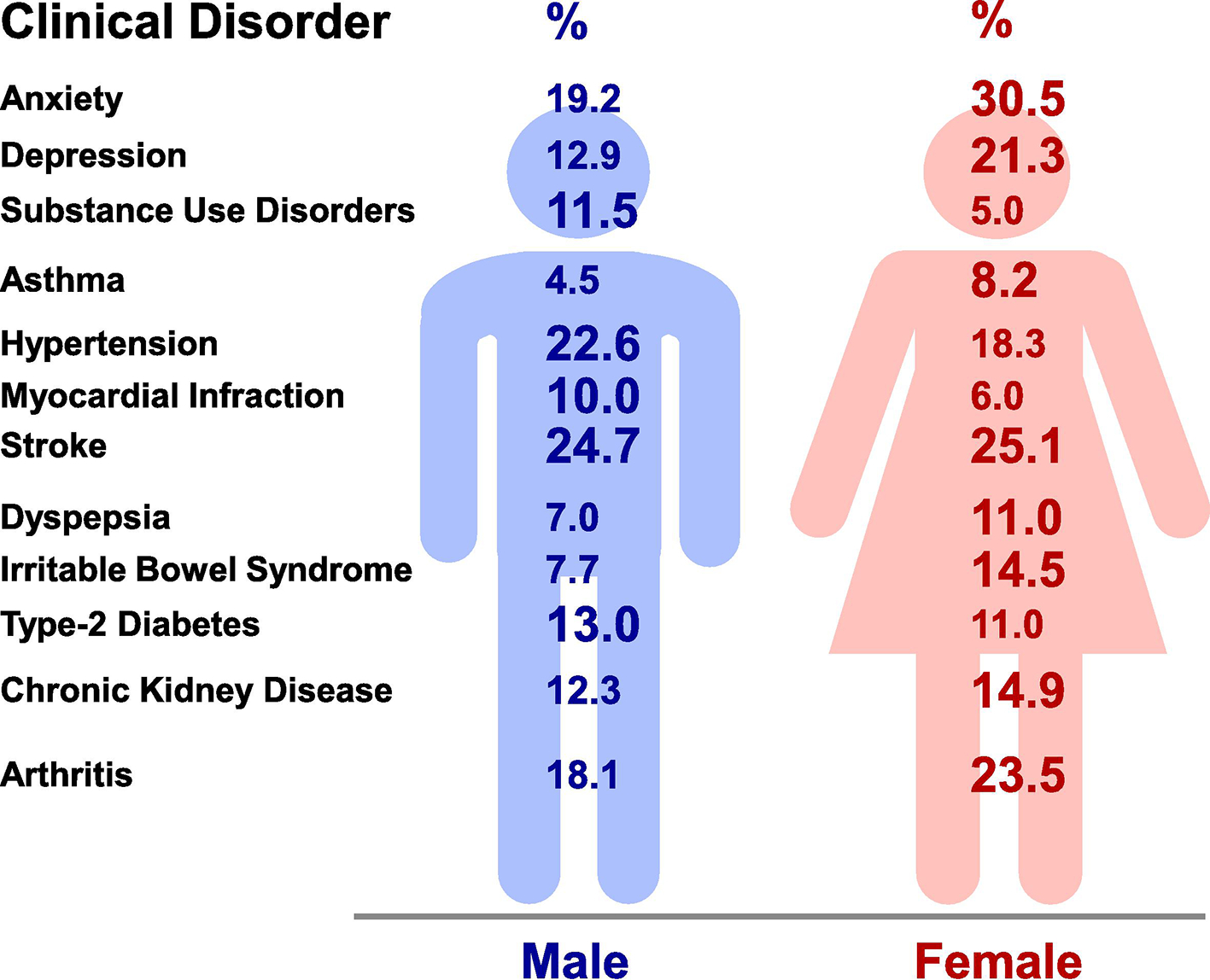
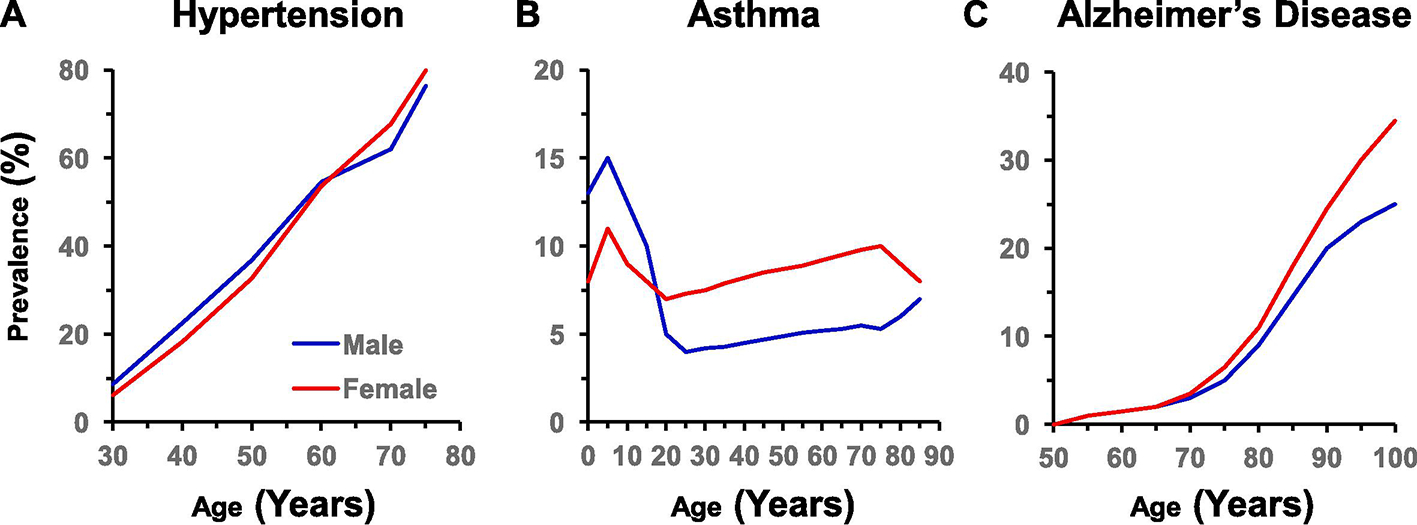
Earlier research has presumed that the male and female biology is similar in most organs except the reproductive system, leading to major misconceptions in research interpretations and clinical implications, with serious disorders being overlooked or misdiagnosed. Careful research has now identified sex differences in the cardiovascular, renal, endocrine, gastrointestinal, immune, nervous, and musculoskeletal systems. Also, several cardiovascular, immunological, and neurological disorders have shown differences in prevalence and severity between males and females. Genetic variations in the sex chromosomes have been implicated in several disorders at young age and before puberty. The levels of the gonadal hormones estrogen, progesterone and testosterone and their receptors play a role in the sex differences between adult males and premenopausal women. Hormonal deficiencies and cell senescence have been implicated in differences between postmenopausal and premenopausal women. Specifically, cardiovascular disorders are more common in adult men vs premenopausal women, but the trend is reversed with age with the incidence being greater in postmenopausal women than age-matched men. Gender-specific disorders in females such as polycystic ovary syndrome, hypertension-in-pregnancy and gestational diabetes have attained further research recognition. Other gender-related research areas include menopausal hormone therapy, the "Estrogen Paradox" in pulmonary arterial hypertension being more predominant but less severe in young females, and how testosterone may cause deleterious effects in the kidney while having vasodilator effects in the coronary circulation. This has prompted the National Institutes of Health (NIH) initiative to consider sex as a biological variable in research. The NIH and other funding agencies have provided resources to establish state-of-the-art centers for women health and sex differences in biology and disease in several academic institutions. Scientific societies and journals have taken similar steps to organize specialized conferences and publish special issues on gender-based research. These combined efforts should promote research to enhance our understanding of the sex differences in biological systems beyond just the reproductive system, and provide better guidance and pharmacological tools for the management of various clinical disorders in a gender-specific manner.
Keywords: Endothelium; Estrogen; Hypertension; Testosterone; Vascular smooth muscle.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
