

Validation of a non-invasive prenatal test for fetal RhD, C, c, E, K and Fya antigens
- PMID: 37550335
- PMCID: PMC10406947
- DOI: 10.1038/s41598-023-39283-3
Validation of a non-invasive prenatal test for fetal RhD, C, c, E, K and Fya antigens
Abstract
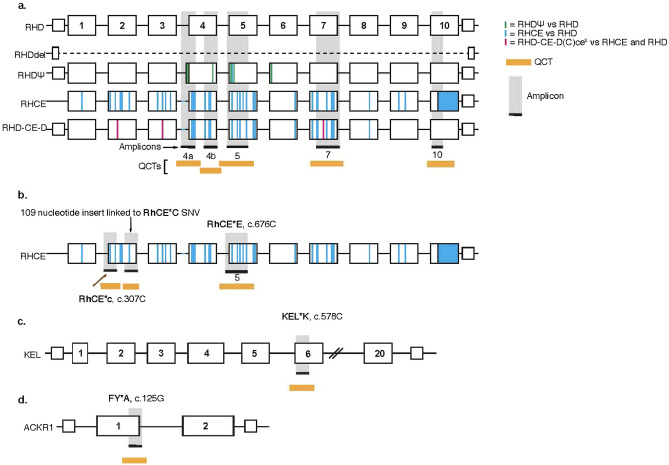
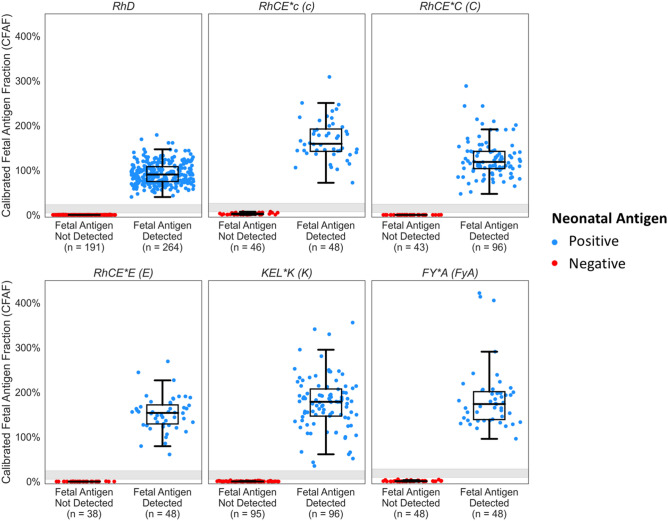
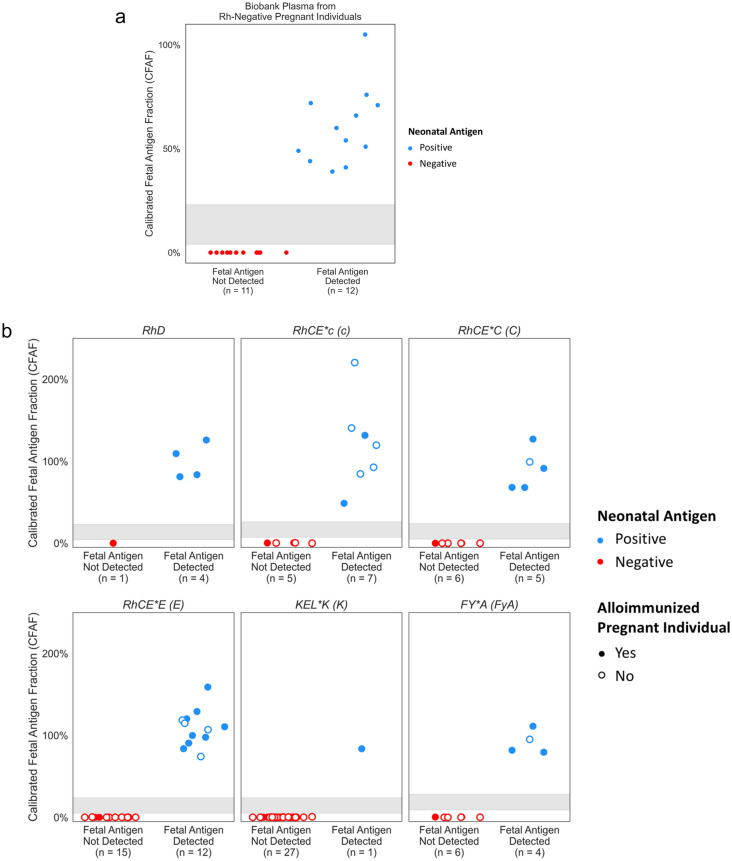
We developed and validated a next generation sequencing-(NGS) based NIPT assay using quantitative counting template (QCT) technology to detect RhD, C, c, E, K (Kell), and Fya (Duffy) fetal antigen genotypes from maternal blood samples in the ethnically diverse U.S. population. Quantitative counting template (QCT) technology is utilized to enable quantification and detection of paternally derived fetal antigen alleles in cell-free DNA with high sensitivity and specificity. In an analytical validation, fetal antigen status was determined for 1061 preclinical samples with a sensitivity of 100% (95% CI 99-100%) and specificity of 100% (95% CI 99-100%). Independent analysis of two duplicate plasma samples was conducted for 1683 clinical samples, demonstrating precision of 99.9%. Importantly, in clinical practice the no-results rate was 0% for 711 RhD-negative non-alloimmunized pregnant people and 0.1% for 769 alloimmunized pregnancies. In a clinical validation, NIPT results were 100% concordant with corresponding neonatal antigen genotype/serology for 23 RhD-negative pregnant individuals and 93 antigen evaluations in 30 alloimmunized pregnancies. Overall, this NGS-based fetal antigen NIPT assay had high performance that was comparable to invasive diagnostic assays in a validation study of a diverse U.S. population as early as 10 weeks of gestation, without the need for a sample from the biological partner. These results suggest that NGS-based fetal antigen NIPT may identify more fetuses at risk for hemolytic disease than current clinical practice, which relies on paternal genotyping and invasive diagnostics and therefore is limited by adherence rates and incorrect results due to non-paternity. Clinical adoption of NIPT for the detection of fetal antigens for both alloimmunized and RhD-negative non-alloimmunized pregnant individuals may streamline care and reduce unnecessary treatment, monitoring, and patient anxiety.
© 2023. Springer Nature Limited.
Conflict of interest statement
B.A., B.P.L, S.H., A.N., X.B., A.B., D.C., J.W., and J.H. are employees of BillionToOne and/or hold stock or options to hold stock in the company. B.H. and J.C. are consultants of BillionToOne. K.J.G. reports consulting fees from BillionToOne, Roche, and Aetion. K.J.G. also reports funding from BillionToOne for the transfer of clinical plasma specimens used in this study. D.E.C and T.F.M report no conflict of interests.
Figures

References
-
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. Number 192: Management of Alloimmunization During Pregnancy. (ACOG, 2018).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
