

Machine learning for genetics-based classification and treatment response prediction in cancer of unknown primary
- PMID: 37550415
- PMCID: PMC11484892
- DOI: 10.1038/s41591-023-02482-6
Machine learning for genetics-based classification and treatment response prediction in cancer of unknown primary
Erratum in
-
Publisher Correction: Machine learning for genetics-based classification and treatment response prediction in cancer of unknown primary.Nat Med. 2024 Feb;30(2):607. doi: 10.1038/s41591-023-02693-x. Nat Med. 2024. PMID: 37968374 No abstract available.
Abstract
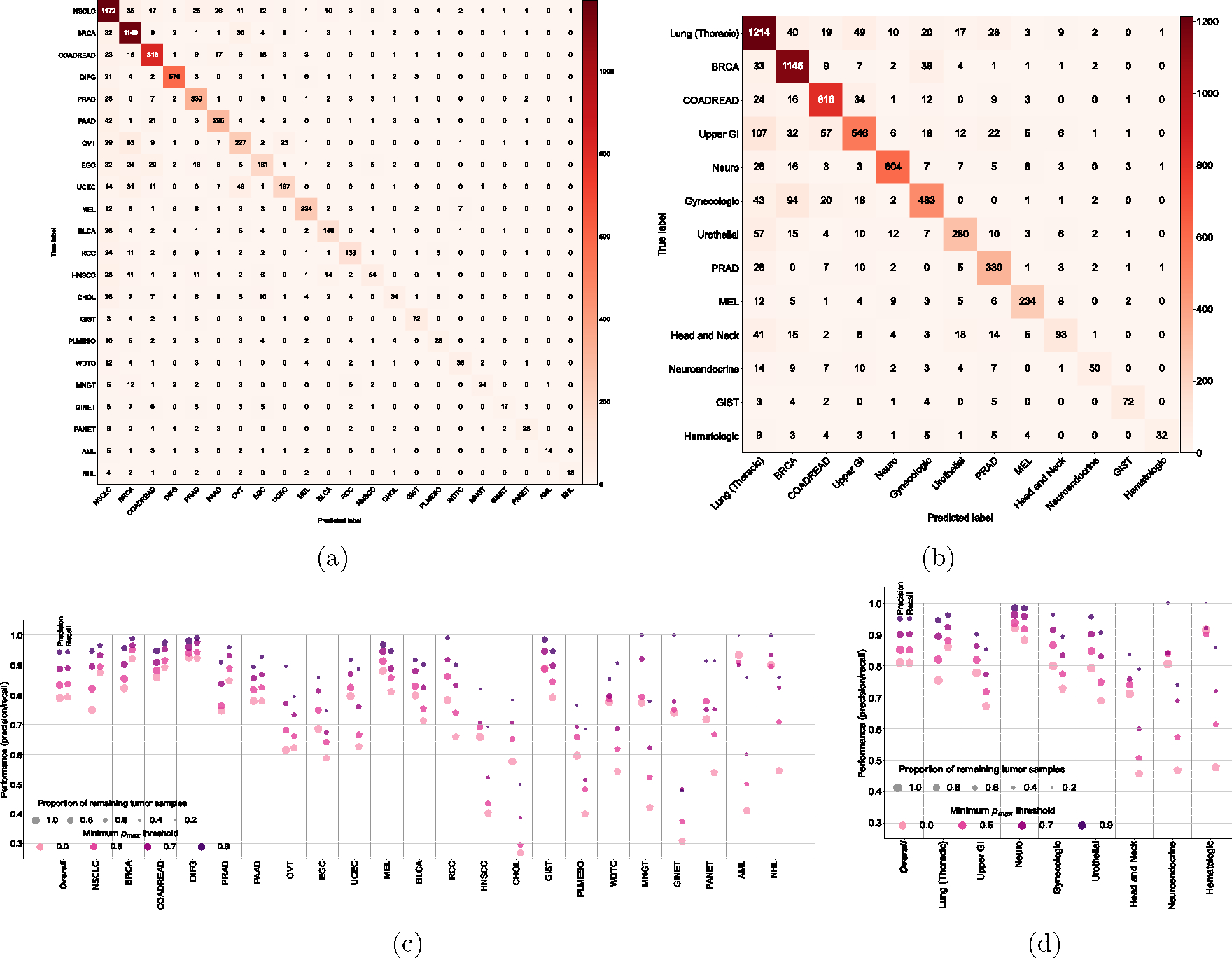
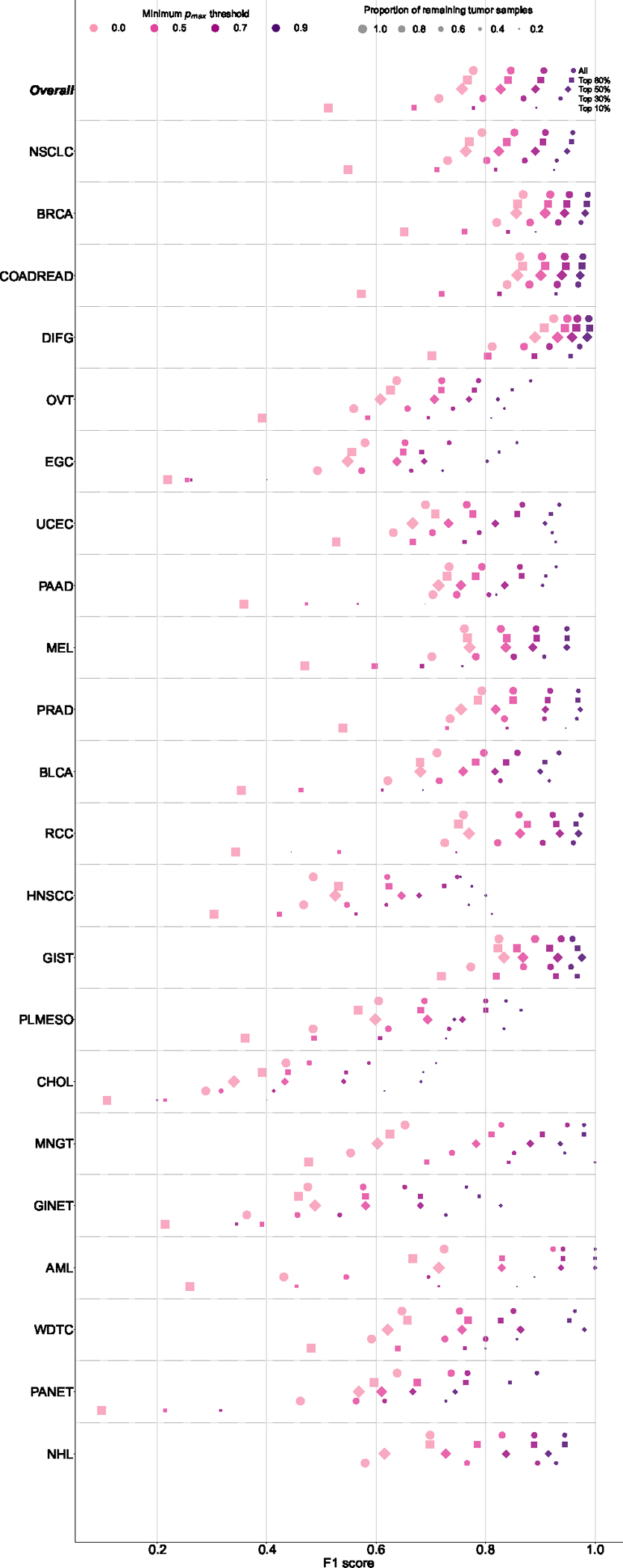
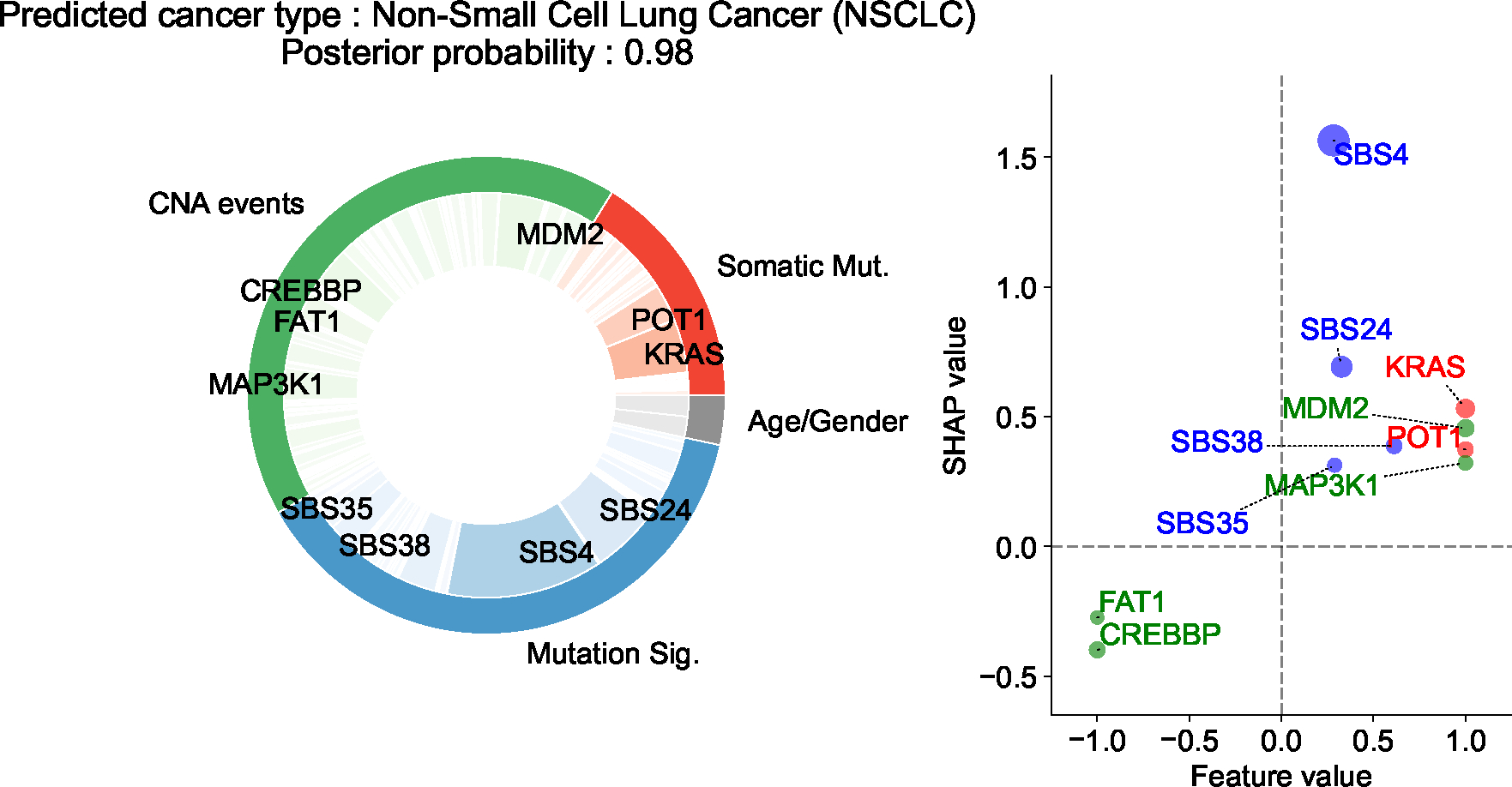
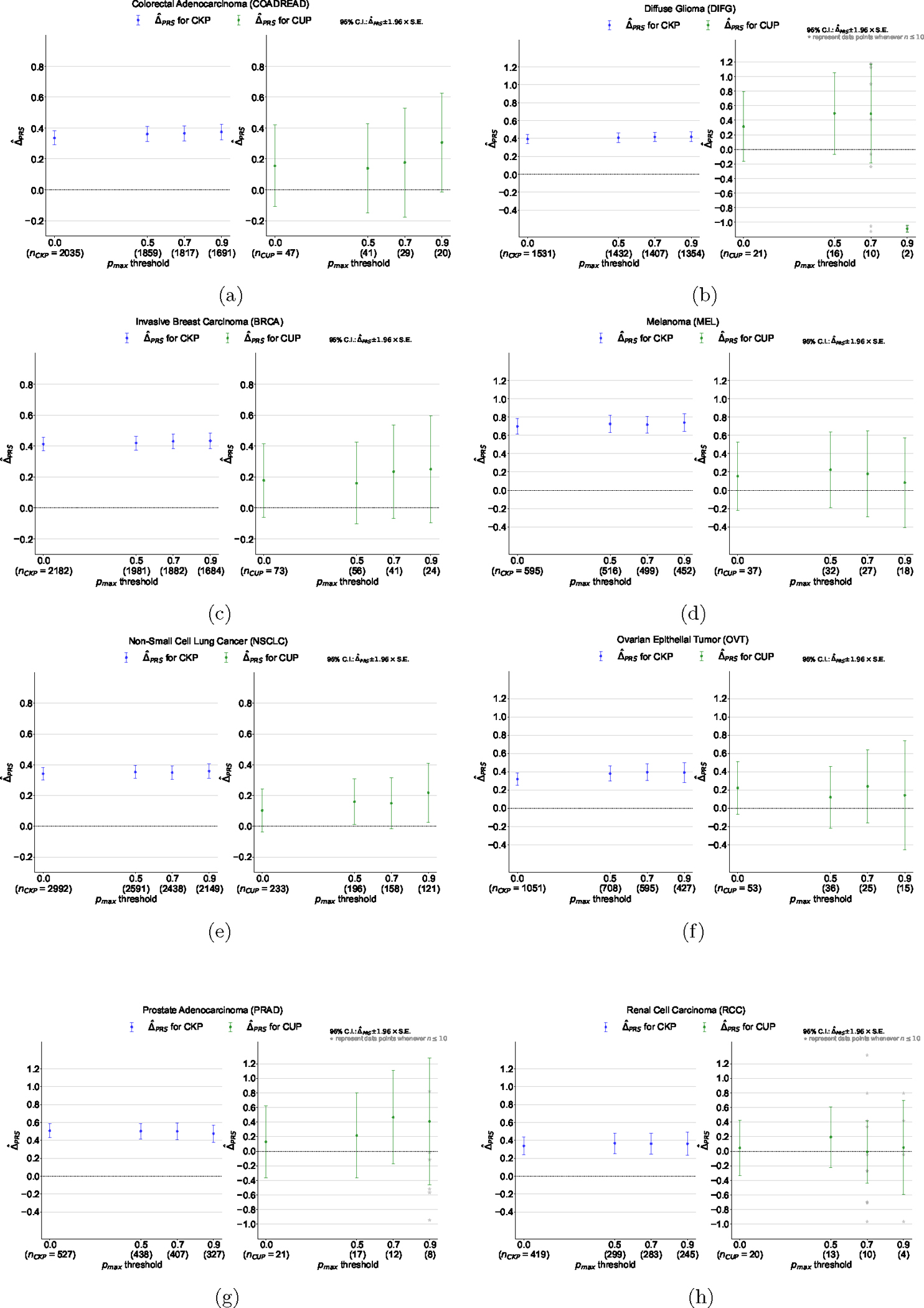
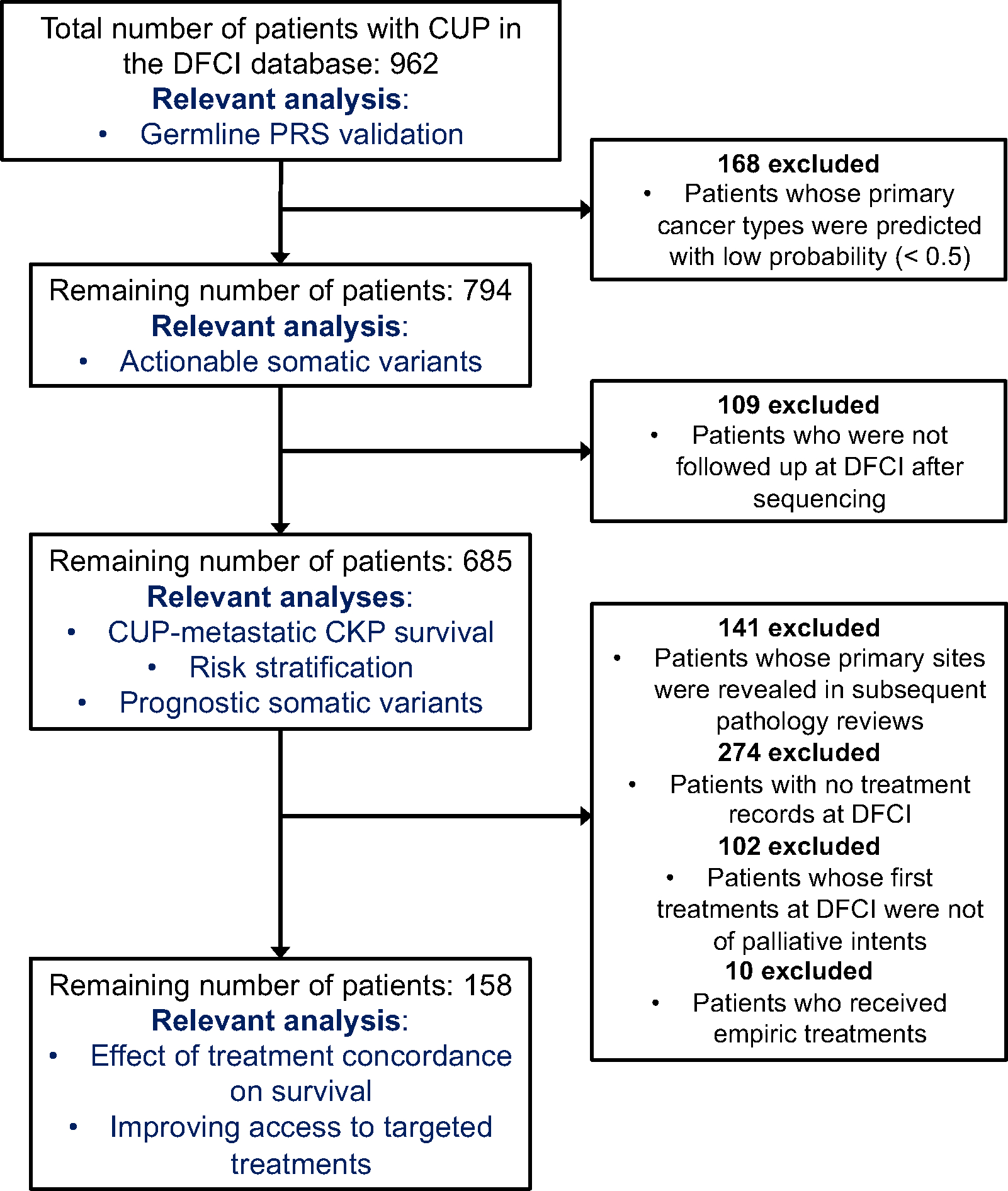
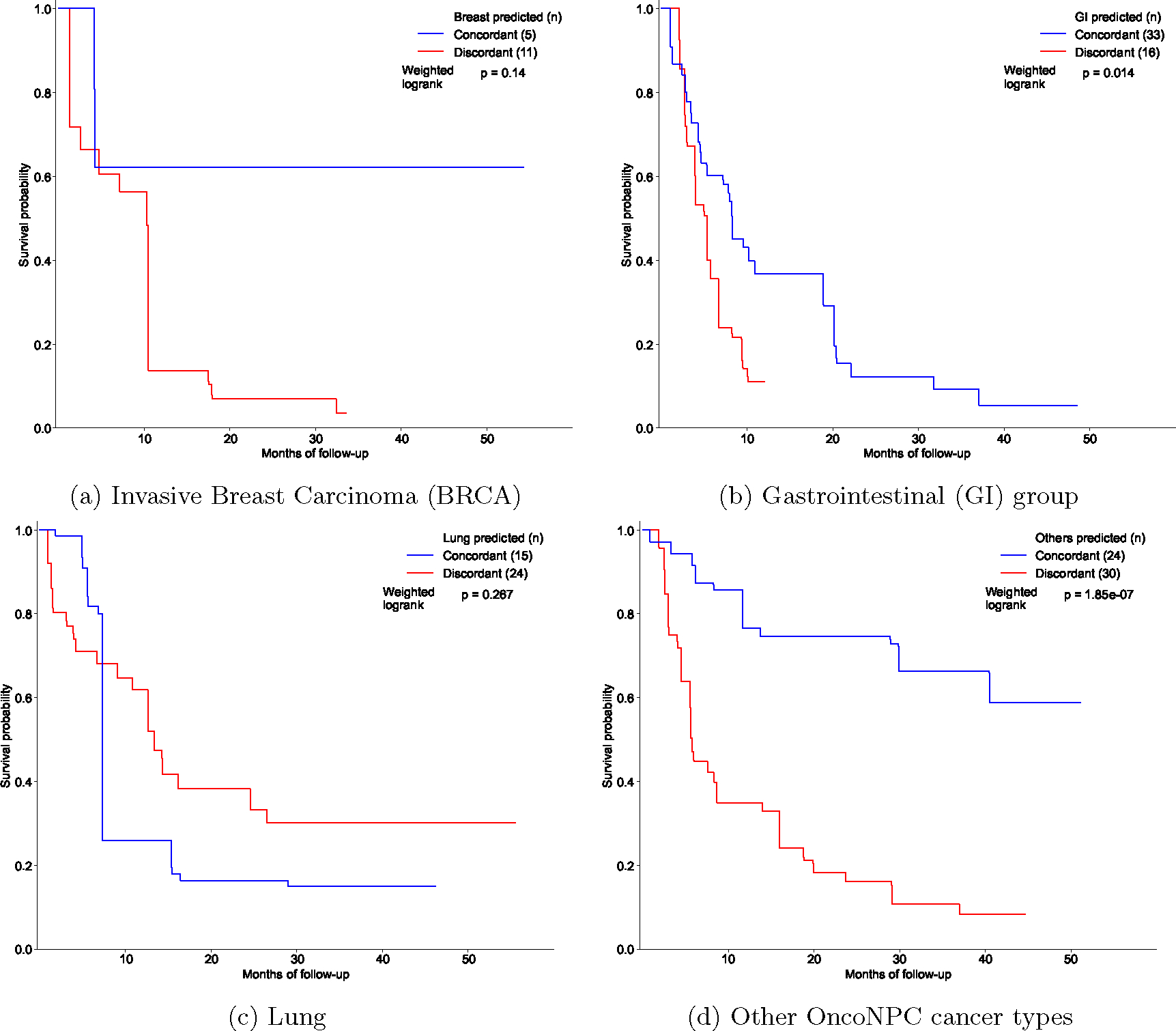
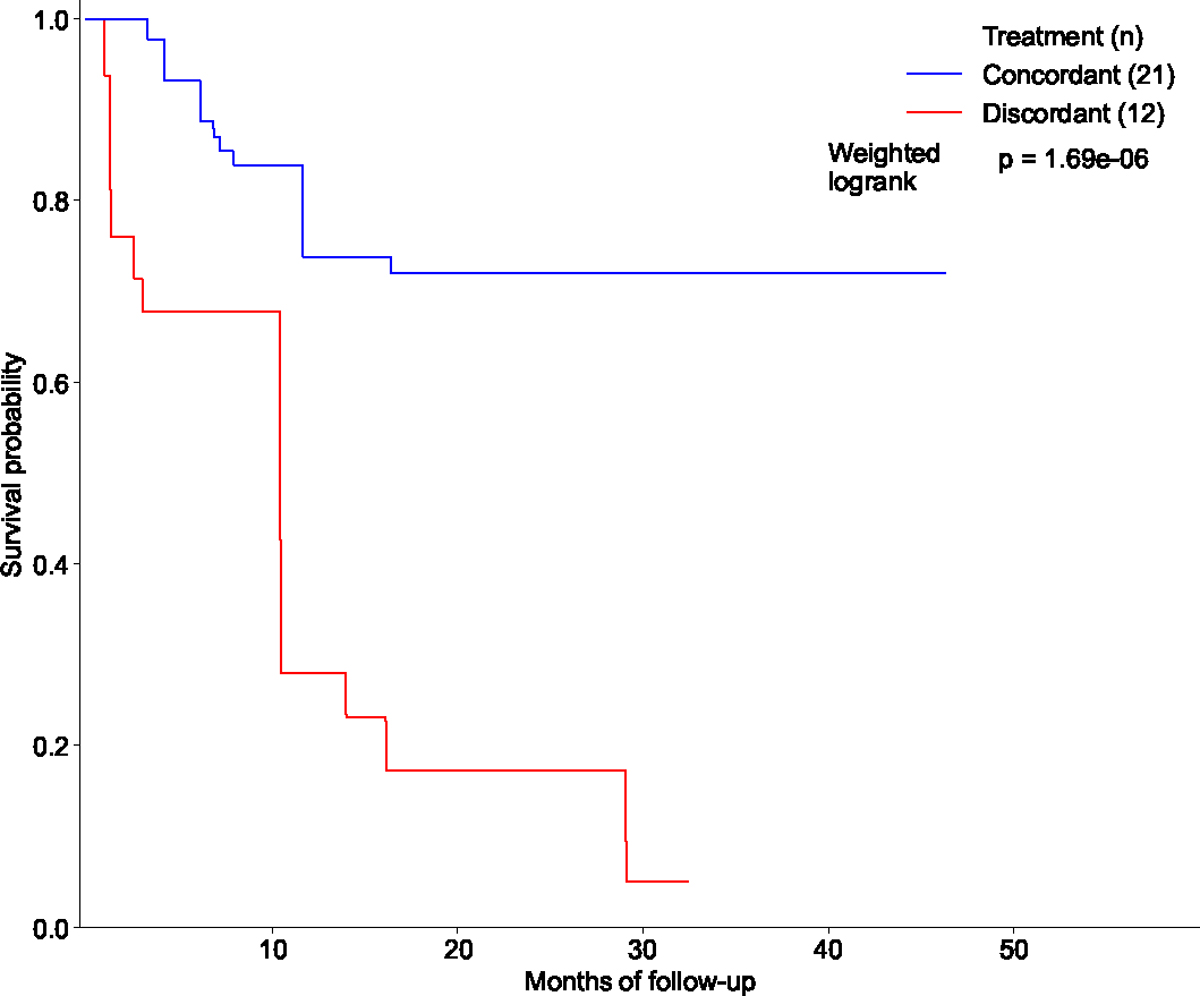
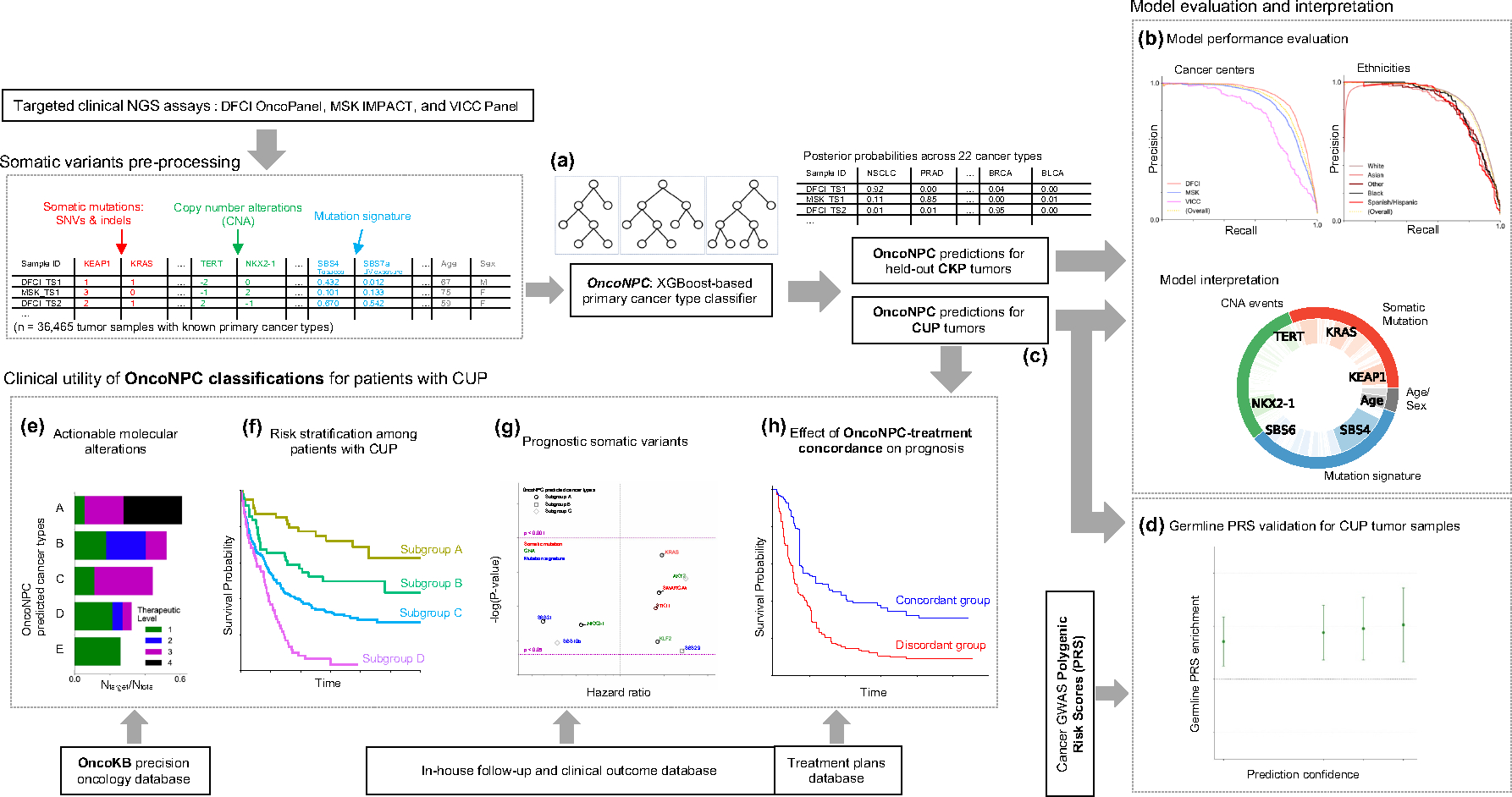
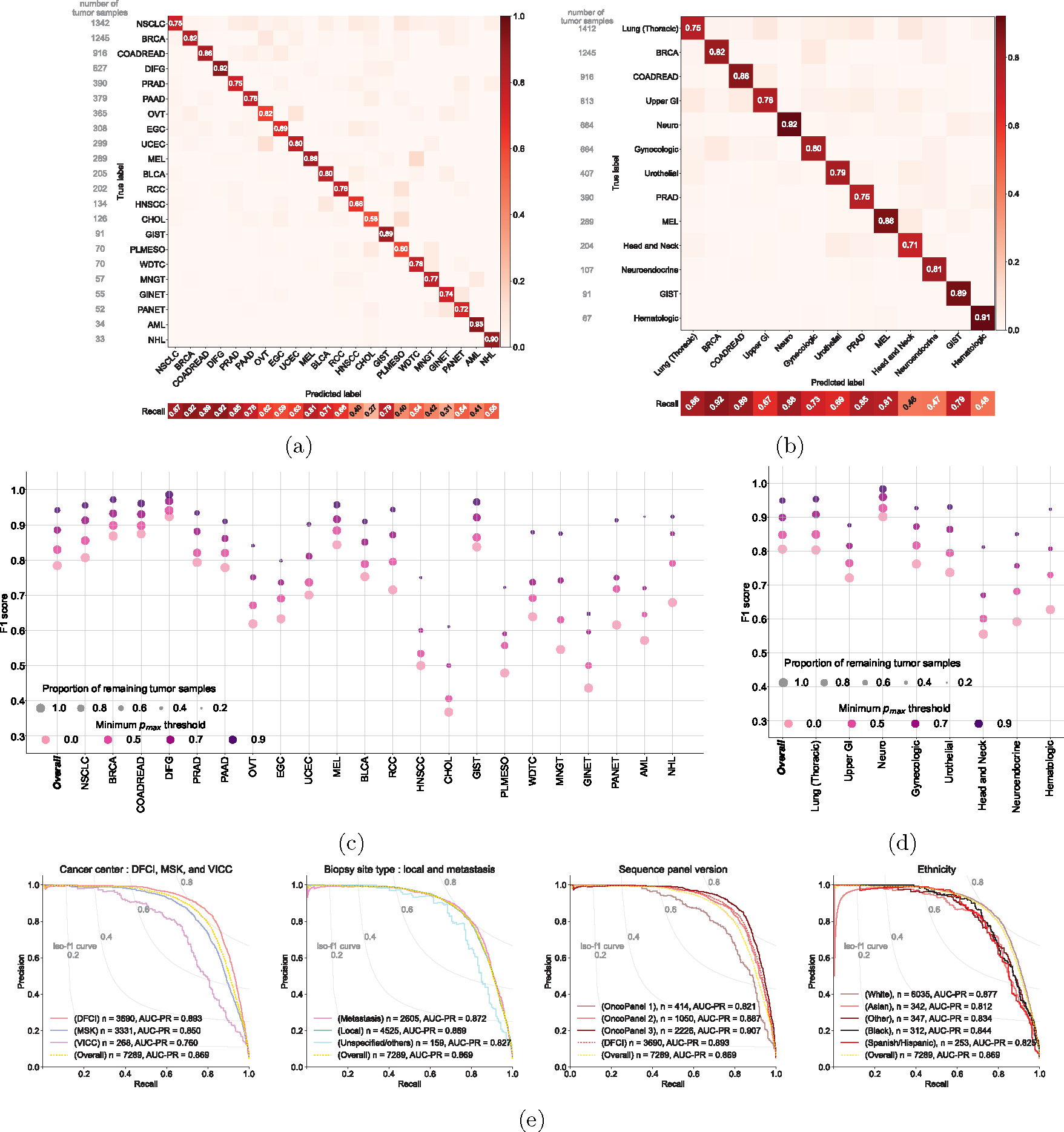
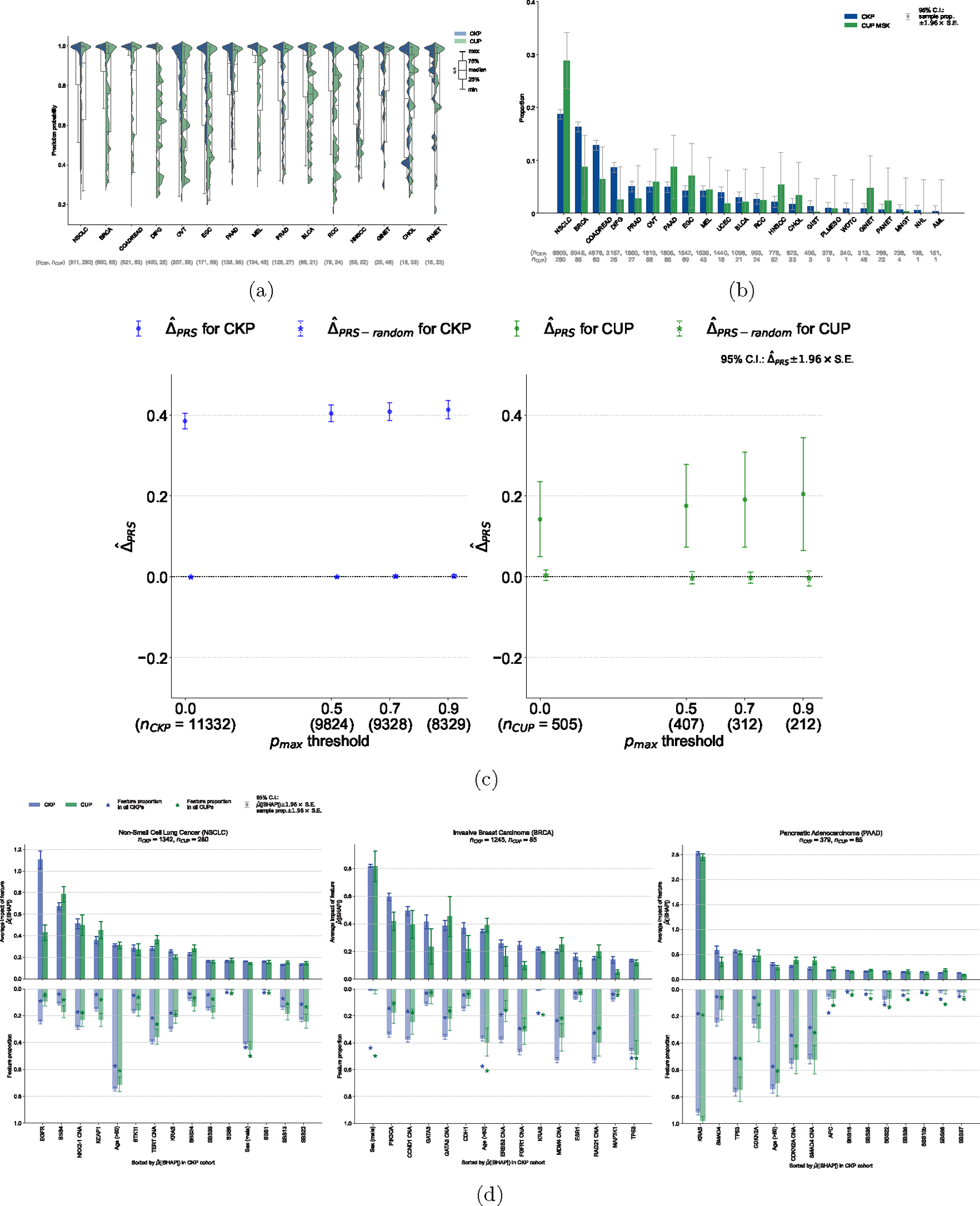
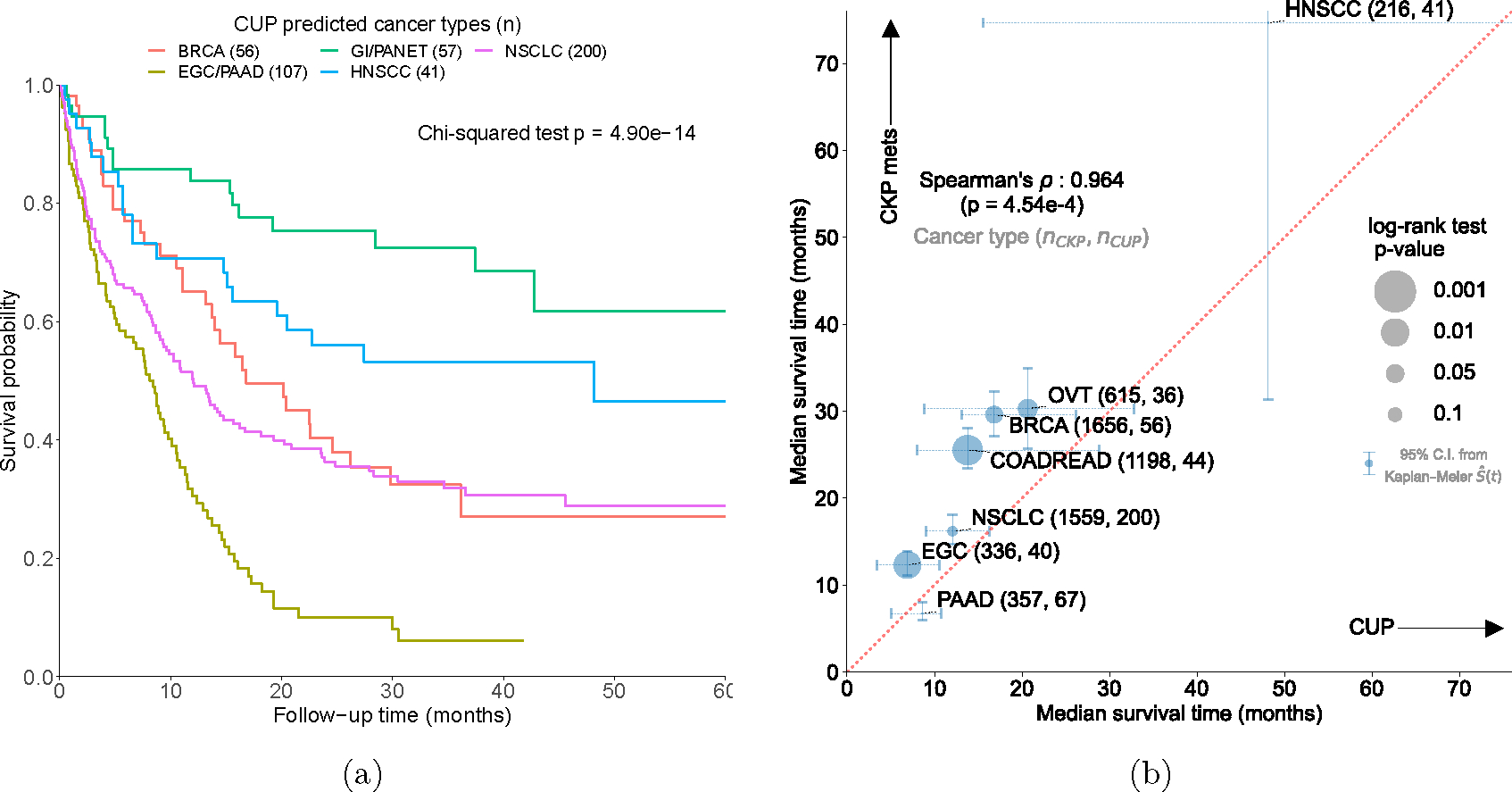
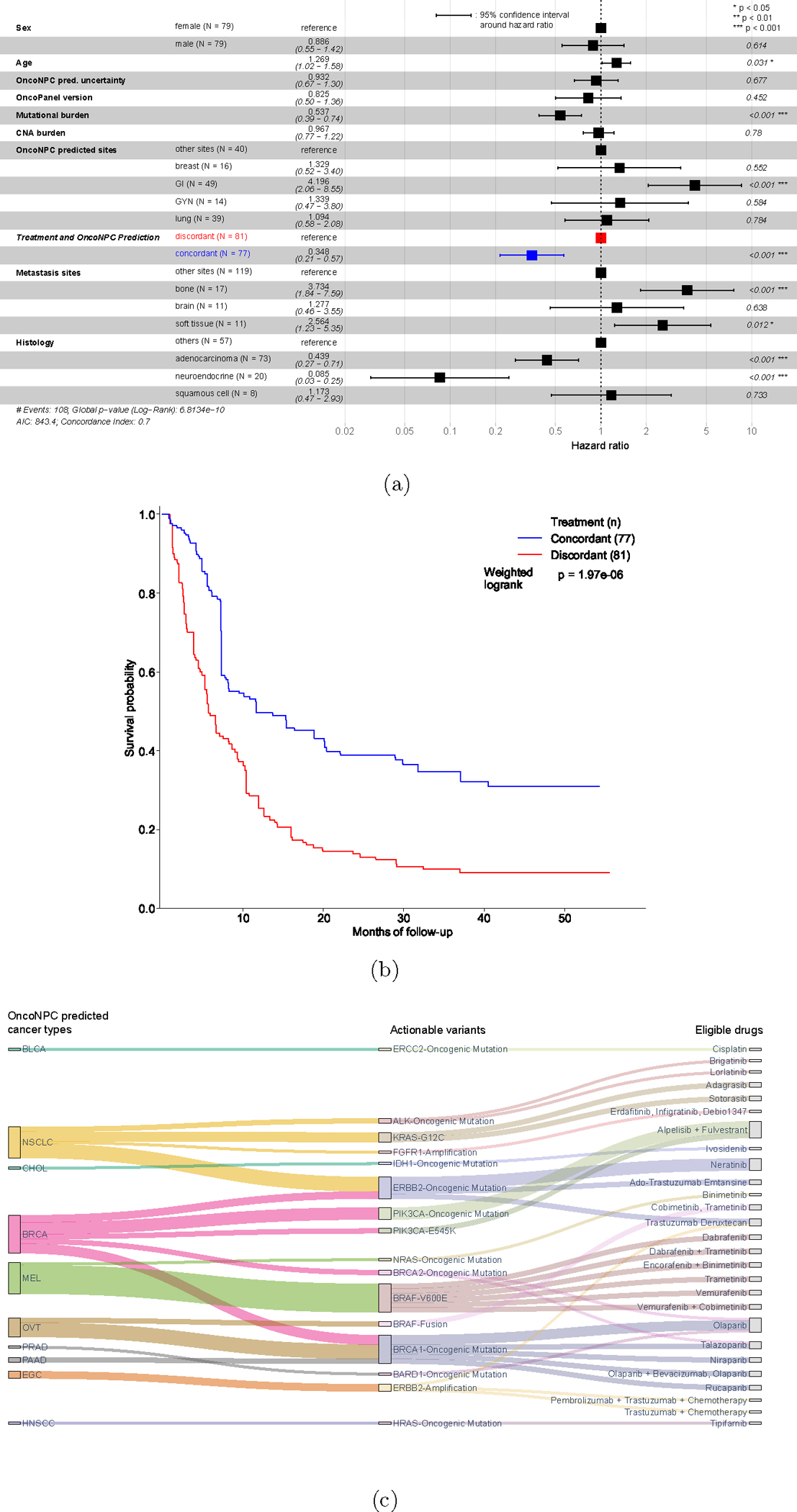
Cancer of unknown primary (CUP) is a type of cancer that cannot be traced back to its primary site and accounts for 3-5% of all cancers. Established targeted therapies are lacking for CUP, leading to generally poor outcomes. We developed OncoNPC, a machine-learning classifier trained on targeted next-generation sequencing (NGS) data from 36,445 tumors across 22 cancer types from three institutions. Oncology NGS-based primary cancer-type classifier (OncoNPC) achieved a weighted F1 score of 0.942 for high confidence predictions ([Formula: see text]) on held-out tumor samples, which made up 65.2% of all the held-out samples. When applied to 971 CUP tumors collected at the Dana-Farber Cancer Institute, OncoNPC predicted primary cancer types with high confidence in 41.2% of the tumors. OncoNPC also identified CUP subgroups with significantly higher polygenic germline risk for the predicted cancer types and with significantly different survival outcomes. Notably, patients with CUP who received first palliative intent treatments concordant with their OncoNPC-predicted cancers had significantly better outcomes (hazard ratio (HR) = 0.348; 95% confidence interval (CI) = 0.210-0.570; P = [Formula: see text]). Furthermore, OncoNPC enabled a 2.2-fold increase in patients with CUP who could have received genomically guided therapies. OncoNPC thus provides evidence of distinct CUP subgroups and offers the potential for clinical decision support for managing patients with CUP.
© 2023. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Competing Interests Statement
The authors declare no competing interests.
Figures


Update of
-
Utilizing Electronic Health Records (EHR) and Tumor Panel Sequencing to Demystify Prognosis of Cancer of Unknown Primary (CUP) patients.Res Sq [Preprint]. 2023 Jan 10:rs.3.rs-2450090. doi: 10.21203/rs.3.rs-2450090/v1. Res Sq. 2023. Update in: Nat Med. 2023 Aug;29(8):2057-2067. doi: 10.1038/s41591-023-02482-6. PMID: 36711812 Free PMC article. Updated. Preprint.
Comment in
-
AI Helps Untangle Cancer Mysteries.Cancer Discov. 2023 Oct 5;13(10):2114. doi: 10.1158/2159-8290.CD-NB2023-0063. Cancer Discov. 2023. PMID: 37638809
References
-
- Varadhachary GR and Raber MN, “Cancer of unknown primary site,” New England Journal of Medicine, vol. 371, no. 8, pp. 757–765, 2014. - PubMed
-
- Hainsworth JD and Greco FA, “Cancer of unknown primary site: New treatment paradigms in the era of precision medicine,” American Society of Clinical Oncology Educational Book, vol. 38, pp. 20–25, 2018. - PubMed
-
- Anderson GG and Weiss LM, “Determining tissue of origin for metastatic cancers: Meta-analysis and literature review of immunohistochemistry performance,” Applied Immunohistochemistry & Molecular Morphology, vol. 18, no. 1, pp. 3–8, 2010. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
