

PECSS: Pulmonary Embolism Comprehensive Screening Score to safely rule out pulmonary embolism among suspected patients presenting to emergency department
- PMID: 37550677
- PMCID: PMC10408070
- DOI: 10.1186/s12890-023-02580-8
PECSS: Pulmonary Embolism Comprehensive Screening Score to safely rule out pulmonary embolism among suspected patients presenting to emergency department
Abstract
Background: Pulmonary embolism is a severe cardiovascular disease and can be life-threatening if left untreated. However, the detection rate of pulmonary embolism using existing pretest probability scores remained relatively low and clinical rule out often relied on excessive use of computed tomographic pulmonary angiography.
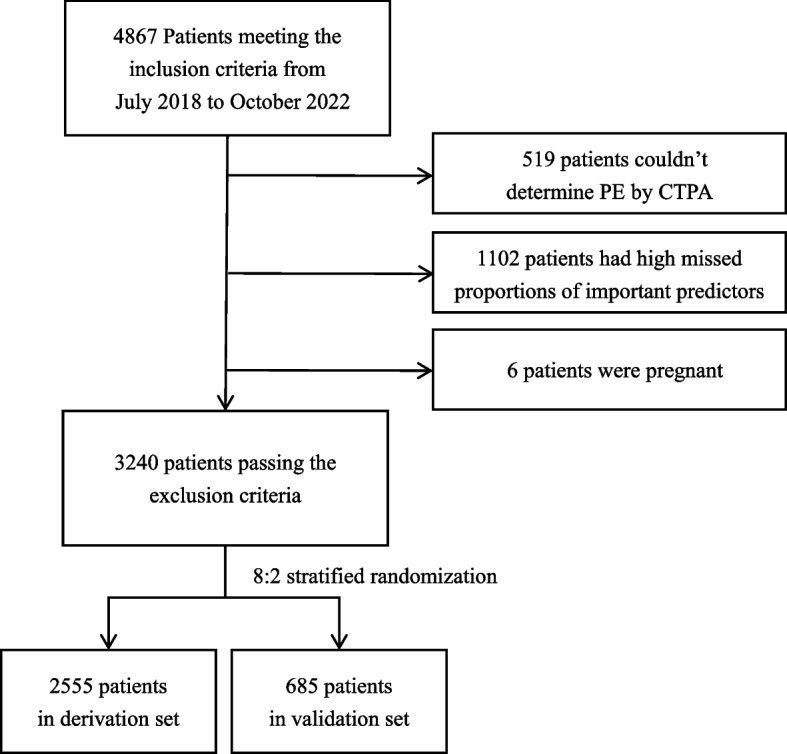
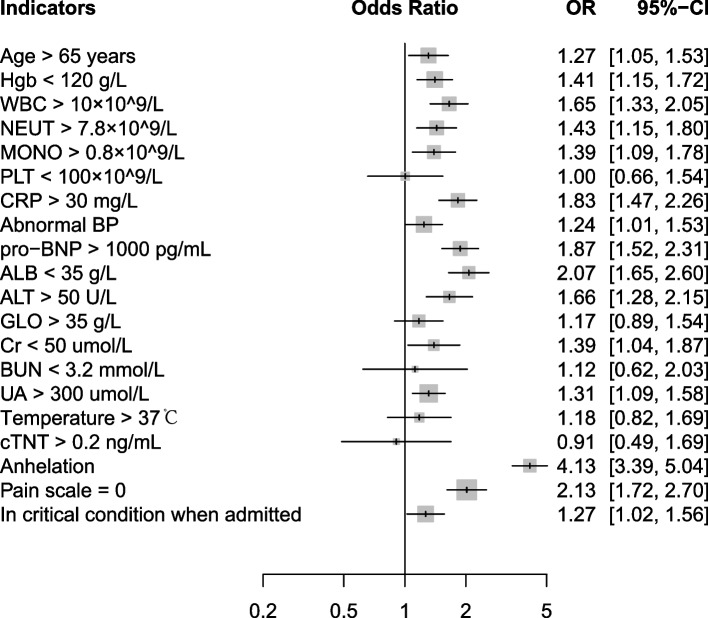
Methods: We retrospectively collected data from pulmonary embolism suspected patients in Zhongshan Hospital from July 2018 to October 2022. Pulmonary embolism diagnosis and severity grades were confirmed by computed tomographic pulmonary angiography. Patients were randomly divided into derivation and validation set. To construct the Pulmonary Embolism Comprehensive Screening Score (PECSS), we first screened for candidate clinical predictors using univariate logistic regression models. These predictors were then included in a searching algorithm with indicators of Wells score, where a series of points were assigned to each predictor. Optimal D-Dimer cutoff values were investigated and incorporated with PECSS to rule out pulmonary embolism.
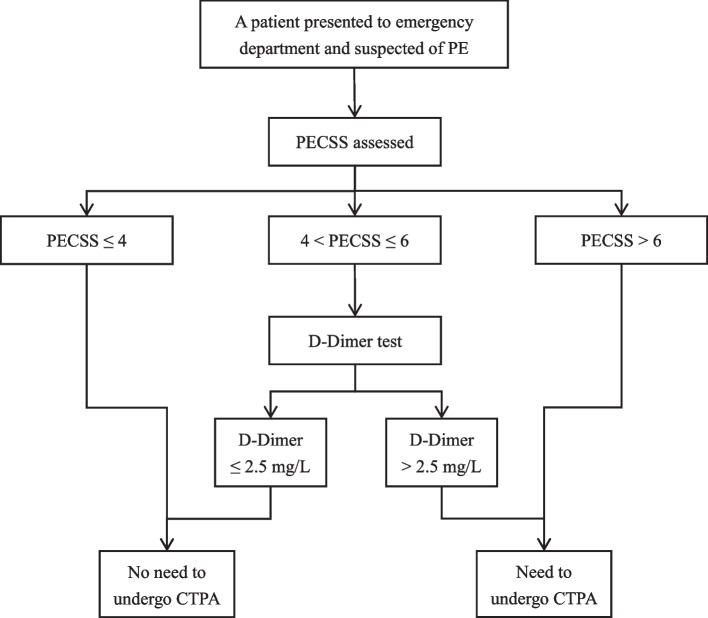
Results: In addition to Wells score, PECSS identified seven clinical predictors (anhelation, abnormal blood pressure, in critical condition when admitted, age > 65 years and high levels of pro-BNP, CRP and UA,) strongly associated with pulmonary embolism. Patients can be safely ruled out of pulmonary embolism if PECSS ≤ 4, or if 4 < PECSS ≤ 6 and D-Dimer ≤ 2.5 mg/L. Comparing with Wells approach, PECSS achieved lower failure rates across all pulmonary embolism severity grades. These findings were validated in the held-out validation set.
Conclusions: Compared to Wells score, PECSS approaches achieved lower failure rates and better compromise between sensitivity and specificity. Calculation of PECSS is easy and all predictors are readily available upon emergency department admission, making it widely applicable in clinical settings.
Trail registration: The study was retrospectively registered (No. CJ0647) and approved by Human Genetic Resources in China in April 2022. Ethical approval was received from the Medical Ethics Committee of Zhongshan Hospital (NO.B2021-839R).
Keywords: D-Dimer; Emergency Department; Pretest probability; Pulmonary Embolism; Screening Score.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
All authors who have taken part in this study declare that they have no competing interest to disclose.
Figures

References
-
- Pollack CV, Schreiber D, Goldhaber SZ, et al. Clinical characteristics, management, and outcomes of patients diagnosed with acute pulmonary embolism in the emergency department: initial report of EMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the Real World Registry) J Am Coll Cardiol. 2011;57(6):700–706. doi: 10.1016/j.jacc.2010.05.071. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
