

The aggregate value of cancer screenings in the United States: full potential value and value considering adherence
- PMID: 37550686
- PMCID: PMC10405449
- DOI: 10.1186/s12913-023-09738-4
The aggregate value of cancer screenings in the United States: full potential value and value considering adherence
Abstract
Background: Although cancer mortality has been decreasing since 1991, many cancers are still not detected until later stages with poorer outcomes. Screening for early-stage cancer can save lives because treatments are generally more effective at earlier than later stages of disease. Evidence of the aggregate benefits of guideline-recommended single-site cancer screenings has been limited. This article assesses the benefits in terms of life-years gained and associated value from major cancer screening technologies in the United States.
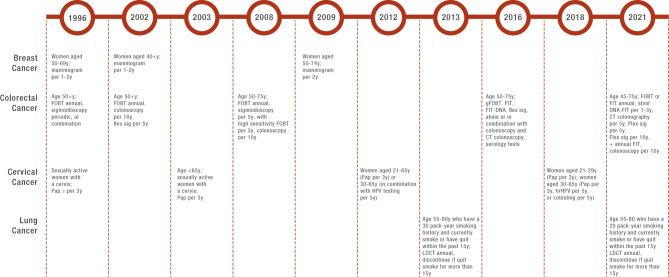
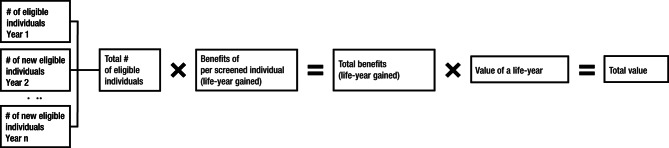
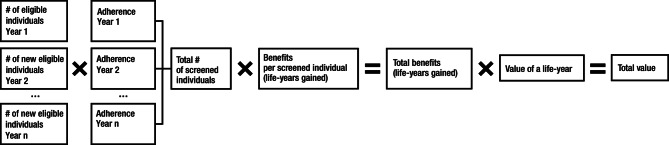
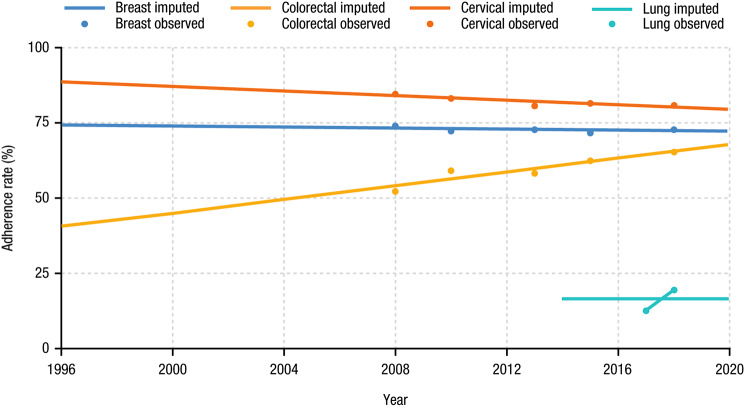
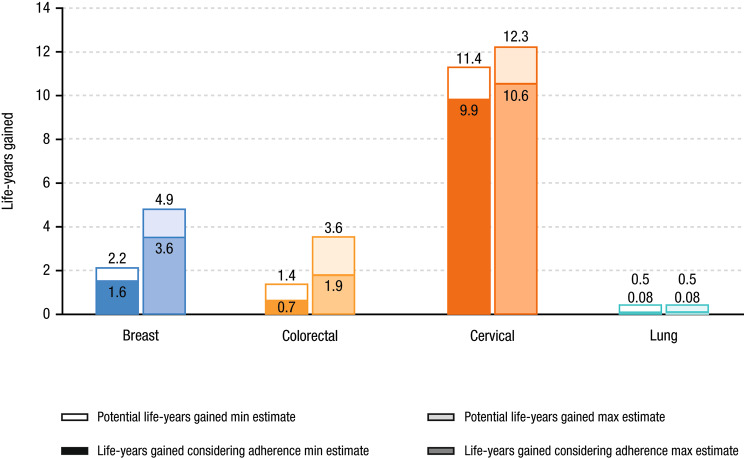
Methods: A mathematical model was built to estimate the aggregate benefits of screenings for breast, colorectal, cervical, and lung cancer over time since the start of US Preventive Services Task Force (USPSTF) recommendations. For each type, the full potential benefits under perfect adherence and the benefits considering reported adherence rates were estimated. The effectiveness of each screening technology was abstracted from published literature on the life-years gained per screened individual. The number of individuals eligible for screening per year was estimated using US Census data matched to the USPSTF recommendations, which changed over time. Adherence rates to screening protocols were based on the National Health Interview Survey results with extrapolation.
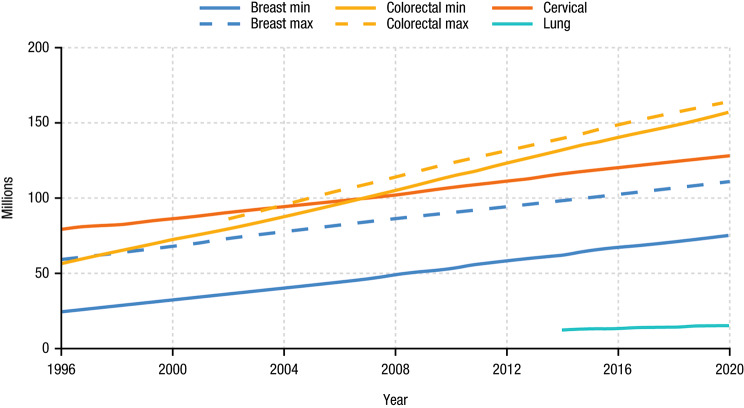
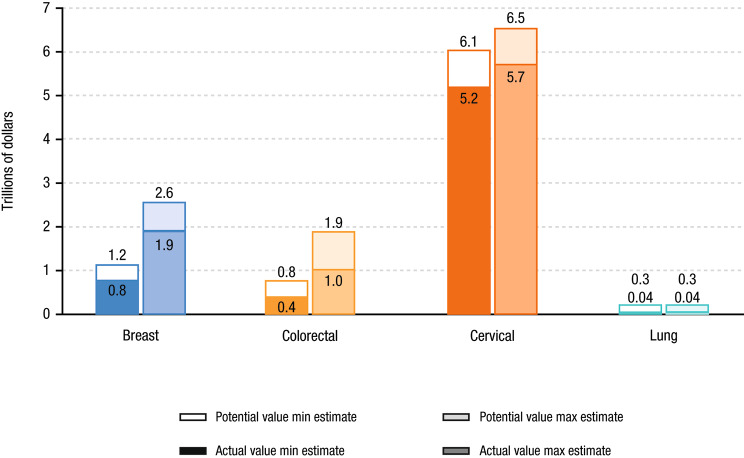
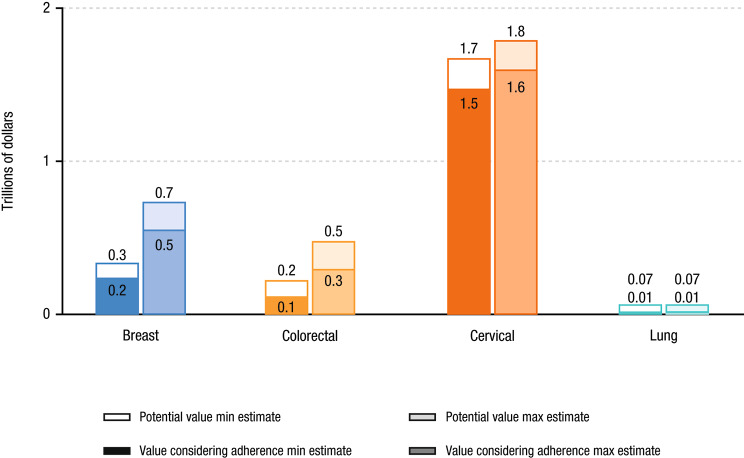
Results: Since initial USPSTF recommendations, up to 417 million people were eligible for cancer screening. Assuming perfect adherence to screening recommendations, the life-years gained from screenings are estimated to be 15.5-21.3 million (2.2-4.9, 1.4-3.6, 11.4-12.3, and 0.5 million for breast, colorectal, cervical, and lung cancer, respectively). At reported adherence rates, combined screening has saved 12.2-16.2 million life-years since the introduction of USPSTF recommendations, ~ 75% of potential with perfect adherence. These benefits translate into a value of $8.2-$11.3 trillion at full potential and $6.5-$8.6 trillion considering current adherence. Therefore, single-site screening could have saved an additional 3.2-5.1 million life-years, equating to $1.7-$2.7 trillion, with perfect adherence.
Conclusions: Although gaps persist between the full potential benefit and benefits considering adherence, existing cancer screening technologies have offered significant value to the US population. Technologies and policy interventions that can improve adherence and/or expand the number of cancer types tested will provide significantly more value and save significantly more patient lives.
Keywords: Cancer screening; Life-years gained; Multi-cancer early detection; Value of cancer screening.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
TP, TD, and AMF received consulting fees from GRAIL LLC. ZC is an employee of Grail LLC.
Figures
References
-
- US Preventive Services Task Force. Davidson KW, Barry MJ, Mangione CM, Cabana M, Caughey AB, Davis EM, Donahue KE, Doubeni CA, Krist AH, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325:1965–77. doi: 10.1001/jama.2021.6238. - DOI - PubMed
-
- Preventive Services Task US, Force, Curry SJ, Krist AH, Owens DK, Barry MJ, Caughey AB, Davidson KW, Doubeni CA, Epling JW, Jr, Kemper AR, et al. Screening for cervical cancer: US preventive services task force recommendation statement. JAMA. 2018;320:674–86. doi: 10.1001/jama.2018.10897. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
