

Does the Ranking Matter? A Retrospective Cohort Study Investigating the Impact of the 2018 CANMAT and ISBD Guidelines for the Management of Patients with Bipolar Disorder Treatment Recommendations for Acute Mania on Rehospitalization Rates
- PMID: 37551100
- PMCID: PMC10411363
- DOI: 10.1177/07067437231156235
Does the Ranking Matter? A Retrospective Cohort Study Investigating the Impact of the 2018 CANMAT and ISBD Guidelines for the Management of Patients with Bipolar Disorder Treatment Recommendations for Acute Mania on Rehospitalization Rates
Abstract
Objective: There is limited data about the impact of mood disorders treatment guidelines on clinical outcomes. The objective of this study was to investigate the impact of prescribers' adherence to the 2018 Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) treatment guidelines recommendations on the readmission rates of patients hospitalized for mania.
Method: A retrospective cohort of all individuals admitted due to acute mania to Kingston General Hospital, Kingston, ON, from January 2018 to July 2021 was included in this study. Patient variables and data regarding index admission and subsequent hospitalizations were extracted from medical records up to December 31, 2021. Treatment regimens were classified as first-line, second-line, noncompliant, or no treatment. We explored the associations between treatment regimens and the risk of readmissions using univariate, multivariate, and survival analysis.
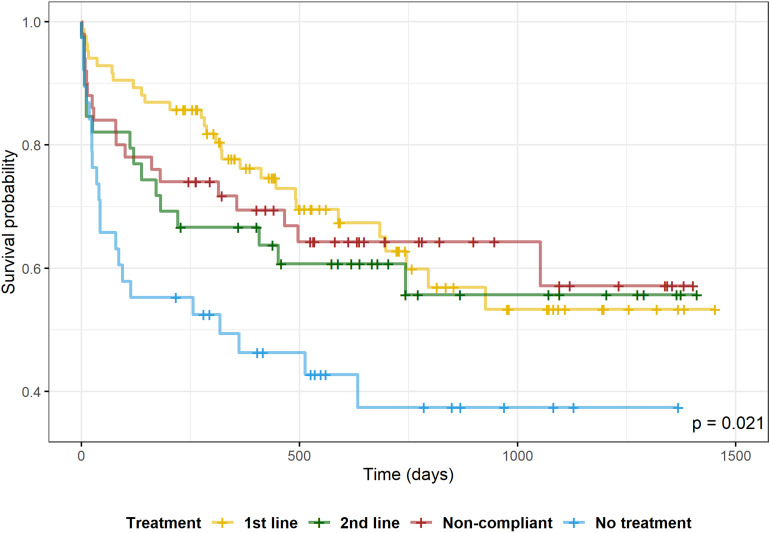
Results: We identified 211 hospitalizations related to 165 patients. The mean time-to-readmission was 211.8 days (standard deviation [SD] = 247.1); the 30-day rehospitalization rate was 13.7%, and any rehospitalization rate was 40.3%. Compared to no treatment, only first-line treatments were associated with a statistically significant decreased risk of 30-day readmission (odds ratio [OR] = 0.209; 95% CI, 0.058 to 0.670). The risk of any readmission was reduced by first-line (OR = 0.387; 95% CI, 0.173 to 0.848) and noncompliant regimens (OR = 0.414; 95% CI, 0.174 to 0.982) compared to no treatment. On survival analysis, no treatment group was associated with shorter time-to-readmission (log-rank test, p = 0.014) and increased risk of readmission (hazard ratio = 2.27; 95% CI, 1.30 to 3.96) when compared to first-line medications.
Conclusions: Treatment with first-line medications was associated with lower 30-day rehospitalization rates and longer time-to-readmission. Physicians' adherence to treatments with higher-ranked evidence for efficacy, safety, and tolerability may improve bipolar disorder outcomes.
Objectif: Il y a des données limitées au sujet de l‘effet des lignes directrices du traitement des troubles de l’humeur sur les résultats cliniques. La présente étude avait comme objectif d’investiguer l’effet de l’adhésion des prescripteurs aux recommandations des lignes directrices de traitement 2018 CANMAT et ISBD concernant les taux de réhospitalisation des patients hospitalisés pour manie.
Méthode: Une cohorte rétrospective de toutes les personnes hospitalisées en raison de manie aiguë à l’Hôpital général de Kingston, ON, de janvier 2018 à juillet 2021 était incluse dans cette étude. Les variables et données des patients concernant la première hospitalisation et les subséquentes ont été extraites des dossiers médicaux jusqu’au 31 décembre 2021. Les régimes de traitement étaient classés ainsi : première ligne, deuxième ligne, non-conforme, ou aucun traitement. Nous avons exploré les associations entre les régimes de traitement et le risque de réhospitalisations à l’aide d’analyse univariée, multivariée et de survie.
Résultats: Nous avons identifié 211 hospitalisations liées à 165 patients. Le temps moyen jusqu’à la réhospitalisation était de 211,8 jours (ET = 247,1); le taux de réhospitalisation de 30 jours était de 13,7 %, et le taux de toute réhospitalisation était de 40,3 %. Comparé à aucun traitement, seuls les traitements de première ligne étaient associés à un risque décru de réhospitalisation de 30 jours (RC 0,209; IC 0,058 à 0,670). Le risque de toute réhospitalisation était réduit par un régime de première ligne (RC 0,387; IC 0,173 à 0,848) et les régimes non conformes (RC 0,414; IC 0,174 à 0,982) comparé à aucun traitement. Dans l’analyse de survie, aucun groupe de traitements n’était associé à un temps plus court jusqu’à la réhospitalisation (test logarithmique par rang, p = 0,014) et à un risque accru de réhospitalisation (rapport de risques 2,27; IC 1,30 à 3,96) quand ils étaient comparés aux médicaments de première ligne.
Conclusions: Le traitement des médicaments de première ligne était associé à des taux plus faibles de réhospitalisation de 30 jours et à des temps plus longs avant la réhospitalisation. L’adhésion des médecins aux traitements indiquant un taux plus élevé d’efficacité, d’innocuité et de tolérabilité peut améliorer les résultats du trouble bipolaire.
Keywords: CANMAT; ISBD; bipolar disorder; clinical guidelines; mania; rehospitalization.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder.Bipolar Disord. 2018 Mar;20(2):97-170. doi: 10.1111/bdi.12609. Epub 2018 Mar 14. Bipolar Disord. 2018. PMID: 29536616 Free PMC article.
-
Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) recommendations for the management of patients with bipolar disorder with mixed presentations.Bipolar Disord. 2021 Dec;23(8):767-788. doi: 10.1111/bdi.13135. Epub 2021 Nov 1. Bipolar Disord. 2021. PMID: 34599629 Review.
-
Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) collaborative update of CANMAT guidelines for the management of patients with bipolar disorder: update 2009.Bipolar Disord. 2009 May;11(3):225-55. doi: 10.1111/j.1399-5618.2009.00672.x. Bipolar Disord. 2009. PMID: 19419382
-
Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) collaborative update of CANMAT guidelines for the management of patients with bipolar disorder: update 2013.Bipolar Disord. 2013 Feb;15(1):1-44. doi: 10.1111/bdi.12025. Epub 2012 Dec 12. Bipolar Disord. 2013. PMID: 23237061
-
The CANMAT and ISBD Guidelines for the Treatment of Bipolar Disorder: Summary and a 2023 Update of Evidence.Focus (Am Psychiatr Publ). 2023 Oct;21(4):344-353. doi: 10.1176/appi.focus.20230009. Epub 2023 Oct 15. Focus (Am Psychiatr Publ). 2023. PMID: 38695002 Free PMC article. Review.
References
-
- Vieta E, Berk M, Schulze TG, et al. Bipolar disorders. Nat Rev Dis Primers. 2018;4(1):18008. - PubMed
-
- McIntyre RS, Berk M, Brietzke E, et al. Bipolar disorders. Lancet. 2020;396(10265):1841–1856. - PubMed
-
- Kessing LV, Hansen MG, Andersen PK. The course of illness in depressive and bipolar disorders. Naturalistic study, 1994–1999. Br J Psychiatry. 2004;185(5):372–377. - PubMed
-
- Verdolini N, Hidalgo-Mazzei D, Del Matto L, et al. Long-term treatment of bipolar disorder type I: a systematic and critical review of clinical guidelines with derived practice algorithms. Bipolar Disord. 2021;23(4):324–340. - PubMed
-
- Institute of Medicine (US) Committee to Advise the Public Health Service on Clinical Practice Guidelines, Field MJ, Lohr KN. (editors). Clinical practice guidelines: directions for a new program. Washington, DC: National Academies Press; 1990. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
