

Systematic Reviews and Meta-analyses of the Procedure-specific Risks of Thrombosis and Bleeding in General Abdominal, Colorectal, Upper Gastrointestinal, and Hepatopancreatobiliary Surgery
- PMID: 37551583
- PMCID: PMC10782937
- DOI: 10.1097/SLA.0000000000006059
Systematic Reviews and Meta-analyses of the Procedure-specific Risks of Thrombosis and Bleeding in General Abdominal, Colorectal, Upper Gastrointestinal, and Hepatopancreatobiliary Surgery
Abstract
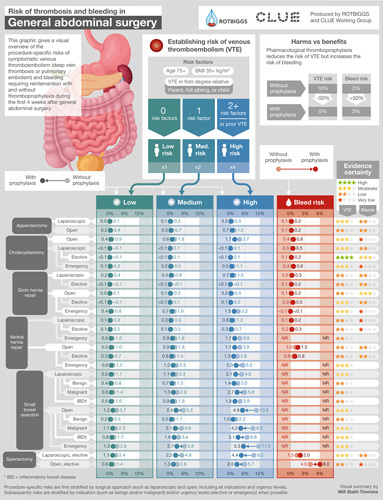
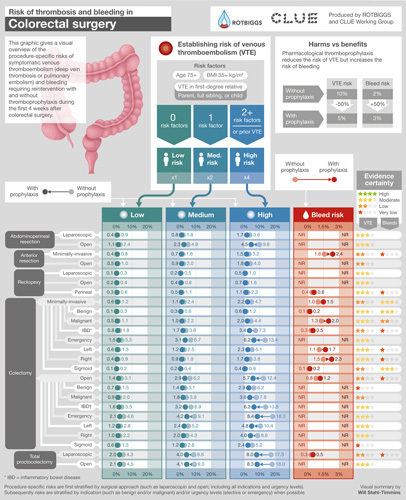
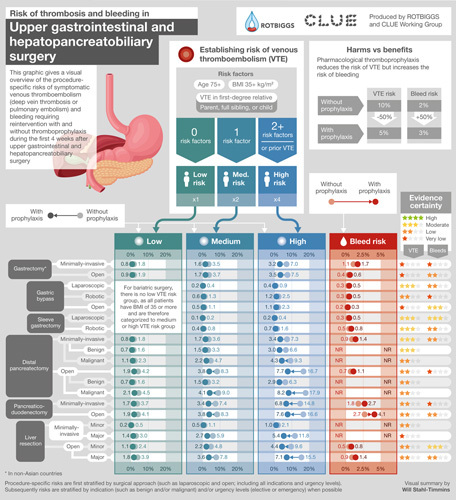
Objective: To provide procedure-specific estimates of symptomatic venous thromboembolism (VTE) and major bleeding after abdominal surgery.
Background: The use of pharmacological thromboprophylaxis represents a trade-off that depends on VTE and bleeding risks that vary between procedures; their magnitude remains uncertain.
Methods: We identified observational studies reporting procedure-specific risks of symptomatic VTE or major bleeding after abdominal surgery, adjusted the reported estimates for thromboprophylaxis and length of follow-up, and estimated cumulative incidence at 4 weeks postsurgery, stratified by VTE risk groups, and rated evidence certainty.
Results: After eligibility screening, 285 studies (8,048,635 patients) reporting on 40 general abdominal, 36 colorectal, 15 upper gastrointestinal, and 24 hepatopancreatobiliary surgery procedures proved eligible. Evidence certainty proved generally moderate or low for VTE and low or very low for bleeding requiring reintervention. The risk of VTE varied substantially among procedures: in general abdominal surgery from a median of <0.1% in laparoscopic cholecystectomy to a median of 3.7% in open small bowel resection, in colorectal from 0.3% in minimally invasive sigmoid colectomy to 10.0% in emergency open total proctocolectomy, and in upper gastrointestinal/hepatopancreatobiliary from 0.2% in laparoscopic sleeve gastrectomy to 6.8% in open distal pancreatectomy for cancer.
Conclusions: VTE thromboprophylaxis provides net benefit through VTE reduction with a small increase in bleeding in some procedures (eg, open colectomy and open pancreaticoduodenectomy), whereas the opposite is true in others (eg, laparoscopic cholecystectomy and elective groin hernia repairs). In many procedures, thromboembolism and bleeding risks are similar, and decisions depend on individual risk prediction and values and preferences regarding VTE and bleeding.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
P.J.K. received a research grant from the Focused Ultrasound Foundation (all unrelated to this manuscript). P.J.D. received research grants from Abbott Laboratories, CloudDX, Philips Healthcare, Roche Diagnostics, and Siemens (all unrelated to this manuscript). R.C., P.D.V., and K.A.O.T. are panel members of the European Society of Anesthesiology and Intensive Care (ESAIC) Task Force for the European Guidelines on Venous Thromboembolism (VTE). The remaining authors report no conflicts of interest.
Figures
Comment in
-
"To bleed or to clot, that is the question"-the benefit of a procedure-specific risk tool to guide perioperative anticoagulation.Hepatobiliary Surg Nutr. 2024 Dec 1;13(6):1058-1061. doi: 10.21037/hbsn-24-608. Epub 2024 Nov 20. Hepatobiliary Surg Nutr. 2024. PMID: 39669071 Free PMC article. No abstract available.
-
Balancing the risks of venous thromboembolism and bleeding in abdominal surgery: factors to consider in personalising thromboprophylaxis.Hepatobiliary Surg Nutr. 2024 Dec 1;13(6):1051-1053. doi: 10.21037/hbsn-24-602. Epub 2024 Nov 15. Hepatobiliary Surg Nutr. 2024. PMID: 39669089 Free PMC article. No abstract available.
References
-
- Research and Markets. General surgery trends and opportunities—procedure volumes analysis—Global 2018. Accessed April 10, 2023. https://www.researchandmarkets.com/reports/4658245/general-surgery-trend...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
